Predicting the Future: Using Simulation Modeling to Forecast Patient Flow on General Medicine Units





BACKGROUND: Hospitals are complex adaptive systems within which multiple components such as patients, practitioners, facilities, and technology interact. A careful approach to optimization of this complex system is needed because any change can result in unexpected deleterious effects. One such approach is discrete event simulation, in which what-if scenarios allow researchers to predict the impact of a proposed change on the system. However, studies illustrating the application of simulation in optimization of general internal medicine (GIM) team inpatient operations are lacking.
METHODS: Administrative data about admissions and discharges, data from a time-motion study, and expert opinion on workflow were used to construct the simulation model. Then, the impact of four changes – aligning medical teams with nursing units, adding a hospitalist team, adding a nursing unit, and adding both a nursing unit and hospitalist team with higher admission volume – were modeled on key hospital operational metrics.
RESULTS: Aligning medical teams with nursing units improved team metrics for aligned teams but shifted patients to unaligned teams. Adding a hospitalist team had little benefit, but adding a nursing unit improved system metrics. Both adding a hospitalist team and a nursing unit would be required to maintain operational metrics with increased patient volume.
CONCLUSION: Using simulation modeling, we provided data on the implications of four possible strategic changes on GIM inpatient units, providers, and patient throughput. Such analyses may be a worthwhile investment to study strategic decisions and make better choices with fewer unintended consequences.
© 2019 Society of Hospital Medicine
METHODS
Setting and Present State
Virginia Commonwealth University (VCU) is a 865-bed tertiary academic medical center, with inpatient care activities spread between four connected buildings and 50 different NUs. The occupancy rate had been over 92% during the time period of this project with admission volume limited primarily by the capacity of the facility. Three of the NUs were primarily allocated to general medicine (GIM) patients. However, over the years, GIM inpatients grew to over 7500 admissions annually, resulting in nearly 50% of GIM patients being admitted to a non-GIM nursing unit.
Additionally, patients on each medical team had a high degree of spread across NUs due to several factors. Admissions and discharges from the hospital did not align across the day. While discharges clumped in the late afternoon, admission occurred throughout the day with a surge in the later afternoon. This mismatch frequently led to patients waiting in the ED for a bed, medical team, or both, and patients were typically assigned to the first available bed and team. For medical team assignments, newly admitted patients were distributed relatively equally across five hospitalist teams and five housestaff teams (that include residents, interns, and medical students). This steady distribution of patients through the day supported meeting housestaff work-hour restrictions of 80 hours each week.18 Yet, as a result of the high occupancy rate, the patterns of patient admissions and discharges, and the distribution of patients among medical teams and across NUs, medical teams and NUs rarely shared more than a few patients.
Leaders at our institution outlined several possible options to address these challenges, including aligning medical teams with NU, adding an additional hospitalist team, or adding an additional nursing unit. In addition, institutional leaders were concerned about the impact of continued growth in admission volume and the impact of patient dispersion on trainees and students. The overall goal of creating a simulation model was to determine the impact of an increased volume of patients and these possible strategic decisions on operational metrics, including number of patients waiting in the ED, ED boarding time per patient, time in system per patient (ED boarding time plus inpatient LOS), team utilization, and rounding travel time.
Simulation Modeling
To model the impact of some possible system changes on patient care, we applied Kelton and Law’s simulation study framework,19 including data collection; model building and validation; and what-if scenario testing (Figure 1).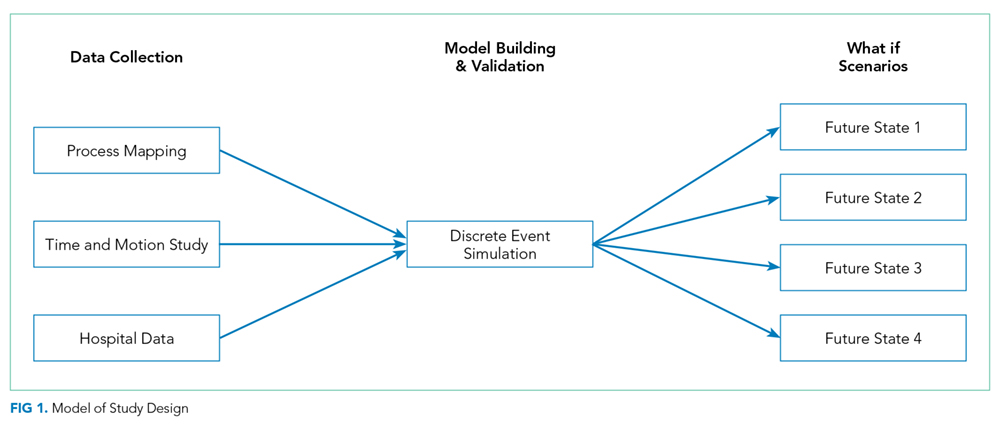
Data Collection
Process Flow Map
We created a complex process flow map of patient care activities on medical teams. The map was developed by four general medicine physicians (R.C., H.M., V.M., and S.P.T.) who all provided medical care on the hospital-based services and ensured expert input on the patient care activities captured by the simulation modeling.
Time and Motion Studies
Time and motion study is a well-established technique used to evaluate the efficiency of work processes.20,21 Originally applied to increase productivity in manufacturing, this technique uses first-hand observations to measure the time allotted to different work tasks to systematically analyze workflow.22 Workflow in healthcare, like manufacturing tasks, tends to have a repetitive pattern, making time and motion studies a highly applicable tool.