Association between Hospitalist Productivity Payments and High-Value Care Culture





BACKGROUND: Given the national emphasis on affordability, healthcare systems expect that their clinicians are motivated to provide high-value care. However, some hospitalists are reimbursed with productivity bonuses and little is known about the effects of these reimbursements on the local culture of high-value care delivery.
OBJECTIVE: To evaluate if hospitalist reimbursement models are associated with high-value culture in university, community, and safety-net hospitals.
DESIGN, PATIENTS, AND SETTINGS: Internal medicine hospitalists from 12 hospitals across California completed a cross-sectional survey assessing their perceptions of high-value care culture within their institutions. Sites represented university, community, and safety-net centers with different performances as reflected by the Centers of Medicare and Medicaid Service’s Value-based Purchasing (VBP) scores.
MEASUREMENT: Demographic characteristics and High-Value Care Culture Survey (HVCCSTM) scores were evaluated using descriptive statistics, and associations were assessed through multilevel linear regression.
RESULTS: Of the 255 hospitalists surveyed, 147 (57.6%) worked in university hospitals, 85 (33.3%) in community hospitals, and 23 (9.0%) in safety-net hospitals. Across all 12 sites, 166 (65.1%) hospitalists reported payment with salary or wages, and 77 (30.2%) with salary plus productivity adjustments. The mean HVCCS score was 50.2 (SD 13.6) on a 0-100 scale. Hospitalists reported lower mean HVCCS scores if they reported payment with salary plus productivity (β = −6.2, 95% CI −9.9 to −2.5) than if they reported payment with salary or wages.
CONCLUSIONS: Hospitalists paid with salary plus productivity reported lower high-value care culture scores for their institutions than those paid with salary or wages. High-value care culture and clinician reimbursement schemes are potential targets of strategies for improving quality outcomes at low cost.
© 2019 Society of Hospital Medicine
Measurement
Hospitalists were asked to complete the High-Value Care Culture Survey (HVCCSTM), which measures the culture of value-based decision making among frontline clinicians.26 Similar to other validated surveys for the assessment of patient safety culture,27,28 the HVCCS can be used to identify target areas for improvement. The survey includes four domains: (1) leadership and health system messaging, (2) data transparency and access, (3) comfort with cost conversations, and (4) blame-free environment. This tool was developed by using a two-phase national modified Delphi process. It was evaluated at two academic centers to complete factor analysis and assess internal consistency, reliability, and validity among internal medicine hospitalists and residents. Validation included estimating product-moment correlation of overall HVCCS scores and domain scores with the CMS institutional VBP scores. HVCCS scores are standardized to a 0-100 point scale for each of the four domains and are then averaged to obtain an overall score.26
In the survey, value was defined as the quality of care provided to patients in relation to the costs required to deliver that care, and high-value care was defined as care that tried to maximize quality while minimizing costs. Quality was defined as the degree to which health services increased the likelihood of desired health outcomes that are safe, effective, patient centered, timely, equitable, and consistent with current professional knowledge. Cost was defined as the negative financial, physical, and emotional effects on patients and the health system.26
Data Analysis
We described the overall institutional mean high-value care culture and domain scores measured by the HVCCS, hospitalist demographics and training experiences, and hospital characteristics. We also described individual survey items. Descriptive statistics were stratified and compared on the basis of hospital type (ie, safety net, community, or university). We assessed the relationship between the clinician perception of reimbursement structure within their divisions and individually reported high-value care culture scores using bivariate and multilevel linear regression. We hypothesized that compared with hospitalists who were paid with salaries or wages, those who reported reimbursement with productivity adjustments may report lower HVCCS scores and those who reported reimbursement with quality or value adjustments may report higher HVCCS scores. We adjusted for physician- and hospital-level characteristics, including age, gender, and training track, and considered hospital type and size as random effects.
This study was approved by the Institutional Review Board at all 12 sites. All analyses were conducted using STATA® 13.0 (College Station, Texas).
RESULTS
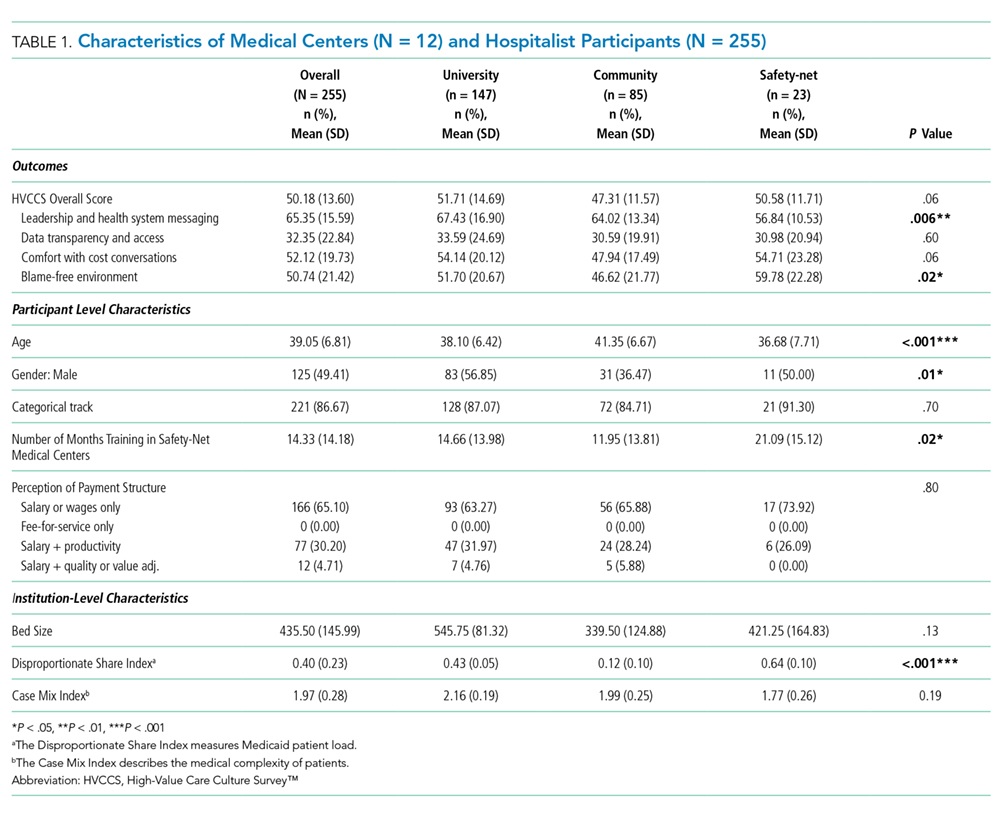
Hospitalist Characteristics
A total of 255 (68.9%, 255/370) hospitalists across all sites completed the survey. Of these respondents, 135 were female (50.6%). On average, hospitalists were 39 years of age (SD 6.8), trained in categorical tracks (221; 86.7%), and had previously trained for 14.3 months at a safety-net hospital (SD 14.2). In total, 166 hospitalists (65.1%) reported being paid with salary or wages, 77 (30.2%) with salary plus productivity adjustments, and 12 (4.7%) with salary plus quality or value adjustments. Moreover, 123 (48.6%) hospitalists agreed that funding for their group depended on the volume of services they delivered. Community-based hospitalists reported higher rates of reimbursement with salary plus productivity (47; 32.0%) compared with their counterparts from university-based (24; 28.2%) and safety-net based programs (6; 26.1%). Among the three different hospital types, significant differences exist in hospitalist mean age (P < .001), gender (P = .01), and the number of months training in a safety-net hospital (P = .02; Table 1).