Predictors of Clinically Significant Echocardiography Findings in Older Adults with Syncope: A Secondary Analysis





BACKGROUND: Syncope is a common reason for visiting the emergency department (ED) and is associated with significant healthcare resource utilization.
OBJECTIVE: To develop a risk-stratification tool for clinically significant findings on echocardiography among older adults presenting to the ED with syncope or near-syncope. DESIGN: Prospective, observational cohort study from April 2013 to September 2016
SETTING: Eleven EDs in the United States
PATIENTS: We enrolled adults (≥60 years) who presented to the ED with syncope or near-syncope who underwent transthoracic echocardiography (TTE).
MEASUREMENTS: The primary outcome was a clinically significant finding on TTE. Clinical, electrocardiogram, and laboratory variables were also collected. Multivariable logistic regression analysis was used to identify predictors of significant findings on echocardiography.
RESULTS: A total of 3,686 patients were enrolled. Of these, 995 (27%) received echocardiography, and 215 (22%) had a significant finding on echocardiography. Regression analysis identified five predictors of significant findings: (1) history of congestive heart failure, (2) history of coronary artery disease, (3) abnormal electrocardiogram, (4) high-sensitivity troponin-T >14 pg/mL, and 5) N-terminal pro B-type natriuretic peptide >125 pg/mL. These five variables make up the ROMEO (Risk Of Major Echocardiography findings in Older adults with syncope) criteria. The sensitivity of a ROMEO score of zero for excluding significant findings on echocardiography was 99.5% (95% CI: 97.4%-99.9%) with a specificity of 15.4% (95% CI: 13.0%-18.1%).
CONCLUSIONS: If validated, this risk-stratification tool could help clinicians determine which syncope patients are at very low risk of having clinically significant findings on echocardiography.
REGISTRATION: ClinicalTrials.gov Identifier NCT01802398.
© 2018 Society of Hospital Medicine
RESULTS
Characteristics of Study Subjects
Patient screening occurred from April 2013 to September 2016. There were 6,930 patients who met eligibility criteria, of whom 3,686 (53%) consented and enrolled in the study (See Figure 1). Of these, 995 (27%) received TTE. The mean age of patients receiving TTE was 74 years; 55% were male. Characteristics of patients obtaining and not obtaining TTE are presented in Appendix Table 2. Patients who received TTE were more likely to be older, have abnormal heart sounds, abnormal EKGs, elevated hs-TnT, elevated NT-proBNP, and have a history of CHF. Of the 995 subjects receiving TTE, 215 (21.6%) had a major, clinically significant finding.
Main Results
Univariate analysis identified 14 variables significantly associated with major findings on TTE. These included male gender, shortness of breath, abnormal heart sounds, history of renal failure, diabetes, CHF, CAD, abnormal ECG, and elevated cardiac biomarkers, among others (See Table 1). The most common major finding on TTE was regional wall motion abnormality, followed by reduced left ventricular ejection fraction (See Table 2). Of the 995 patients who received TTE, 20 (2%) were discharged directly from the ED, 444 (45%) were observed, and 531 (53%) were admitted. On average, patients who received TTE had a longer length of stay than did those that did not (3.4 days vs 1.9 days).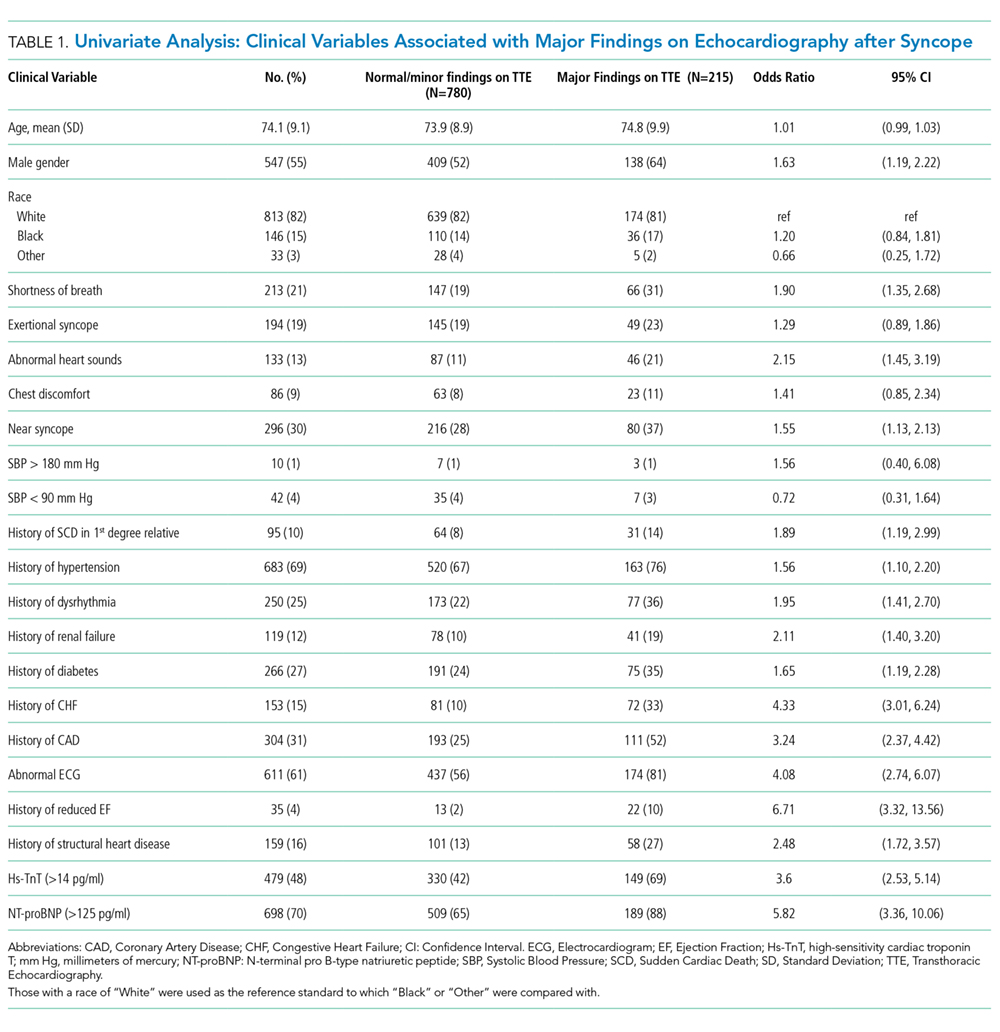
LASSO multivariable logistic regression produced five predictors associated with major findings on TTE: 1) history of CHF, 2) history of CAD, 3) abnormal ECG, 4) hs-TnT above 14 pg/mL, and 5) NT-proBNP above 125 pg/mL (See Table 3).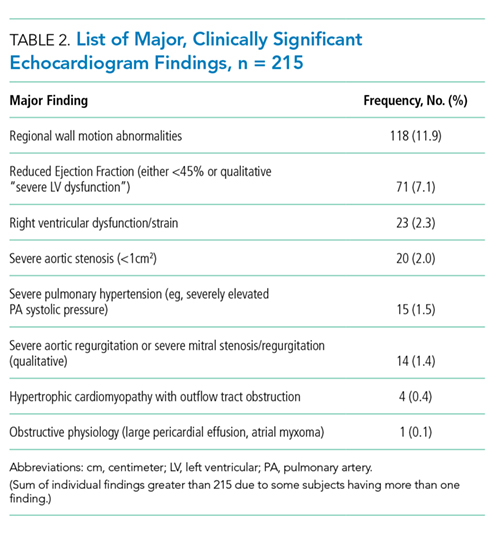
These five high-risk clinical variables retained their importance after multivariate analysis and form the ROMEO score.
The sensitivity and specificity of a ROMEO score of zero for excluding major findings on TTE was 99.5% (95% CI: 97.4%-99.9%) and 15.4% (95% CI: 13.0%-18.1%), respectively. Patients with a ROMEO score of 0 were at very low risk of having a major finding on TTE: 0.8% (95% CI: 0.02%-4.5%; Appendix Table 3). Only one out of 121 patients with none of the ROMEO criteria was found to have a major finding on TTE (regional wall motion abnormality). Patients with a score of 1 or more were at moderate-to-high risk of having a major finding (7.3% to 55.6%).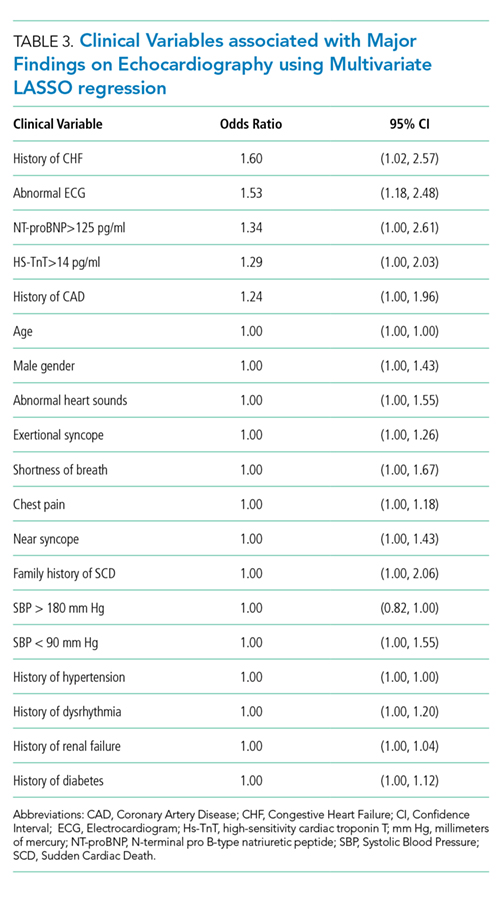
There was a linear relationship between the ROMEO score and probability of major findings on TTE (See Appendix Figure 1). The AUC was 0.77 (95% CI = 0.72-0.79) indicating good accuracy of the combination of the five high-risk clinical variables to predict major findings on TTE (See Appendix Figure 2). After excluding the 72 patients with known CHF and significant findings on TTE, the AUC was similar: 0.73 (95% CI: 0.69-0.77). There were 139 patients with at least one missing variable (14%) (See Appendix Table 4). A multiple imputation sensitivity analysis identified the same five high-risk clinical variables in 85% of imputations.
There were 253 patients with high-sensitivity troponin levels between 15 and 30 pg/mL (inclusive). Using a higher hs-TnT threshold (>30 pg/mL) to simulate a conventional troponin assay again identified the same five high-risk variables along with shortness of breath as a potential sixth variable though with an odds ratio approaching unity (See Appendix Table 5). The ROMEO score would have missed two additional patients with major findings if the troponin cutoff were raised to 30 pg/mL from 14 pg/mL, ie, it would have identified 212/215 (98.6%) of the major findings rather than 214/215 (99.5%).
