An Electronic Health Record Tool Designed to Improve Pediatric Hospital Discharge has Low Predictive Utility for Readmissions





We developed an electronic health record tool to improve pediatric hospital discharge. This tool flags children with three components that might complicate discharge: home health, polypharmacy (≥6 medications), or non-English speaking caregiver. The tool tallies components and displays them as a composite score of 0-3 points. We describe the tool’s development, implementation, and an evaluation of its predictive utility for 30-day unplanned readmissions in 29,542 discharged children. Of these children, 28% had a composite score of 1, 8% a score ≥2, and 4% were readmitted. The odds of readmission was significantly higher in children with composite score of 1 versus 0 (odds ratio [OR]: 1.7; 95% CI, 1.5-2) and ≥2 versus 0 (OR 4.2; 95% CI 3.6-4.9). The C-statistic for this model was 0.62. Despite the positive association of the score with readmission, the tool’s discriminatory performance is low. Additional research is needed to evaluate its practical benefit for improving the quality of hospital discharge.
© 2018 Society of Hospital Medicine
RESULTS
Cohort Characteristics
Analysis was restricted to 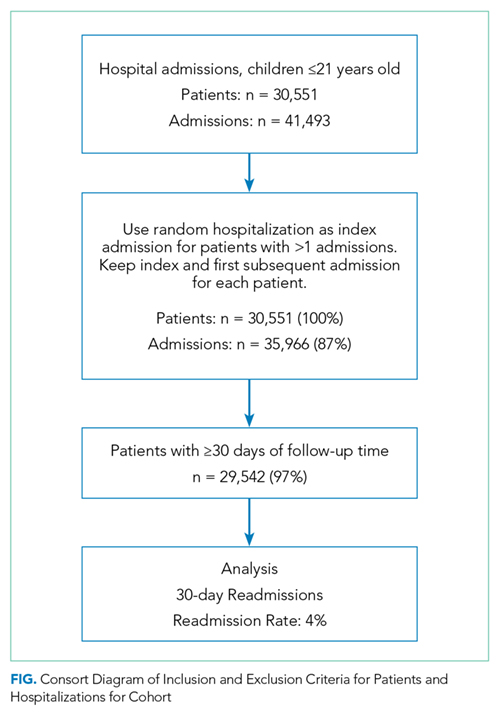
ROC analysis indicated that dichotomizing number of medications at ≥6 vs. <6 and home health at 0 vs. ≥1 categories maximized the sensitivity and specificity for predicting 30-day unplanned readmissions. In predictive logistic regression analysis, the odds of readmission was significantly higher in children with a composite score of 1 vs. 0 (odds ratio [OR], 1.7; 95% CI 1.5-2) and a score of ≥2 vs. 0 (OR, 4.2; 95% CI, 3.6-4.9). The c statistic for this model was 0.62, and the Brier score was 0.037. Internal validation of the predictive logistic regression model yielded identical results.
DISCUSSION
The instrument’s framework is relatively simple and should reduce barriers to implementation elsewhere. However, this tool was developed for one setting, and the design may require adjustment for other environments. Regional or institutional variation in home-health eligibility or clinical documentation may impact home-care and medication scores. The score may change at discharge if home-health or medication orders are modified late. The tool performs none of the following: measurement of regimen complexity, identification of high-risk medications, distinguishing of new versus preexisting medications/home care, nor measurement of health literacy, parent education, or psychosocial risk. Adding these features might enhance the model. Finally, readmission rates did not rise linearly with each added point. A more sophisticated scoring system (eg, differentially weighting each risk factor) may also improve the performance of the tool.
Despite these limitations, we have implemented a real-time electronic tool with practical potential to improve the discharge process but with low utility for distinguishing readmissions. Additional validation and research is needed to evaluate its impact on hospital discharge quality metrics and family reported outcome measures.