Does Patient Experience Predict 30-Day Readmission? A Patient-Level Analysis of HCAHPS Data





BACKGROUND: Hospital-level studies have found an inverse relationship between patient experience and readmissions. However, based on typical survey response time, it is unclear if patients are able to respond to surveys before they get readmitted and whether being readmitted might be a driver of poor experience scores (reverse causation).
OBJECTIVE: Using patient-level Hospital Consumer Assessment of Healthcare Providers and Systems (HCHAPS) and Press Ganey data to examine the relationship between readmissions and experience scores and to distinguish between patients who responded before or after a subsequent readmission. DESIGN: Retrospective analysis of 10-year HCAHPS data.
SETTING: Single tertiary care academic hospital.
PARTICIPANTS: Patients readmitted within 30 days of an index hospitalization who received an HCAHPS survey linked to index admission comprised the exposure group. This group was divided into those who responded prior to readmission and those who responded after readmission. Nonreadmitted patients comprised the control group.
ANALYSIS: Multivariable-logistic regression to analyze the association between HCHAPS and Press Ganey scores and 30-readmission status, adjusted for patient factors.
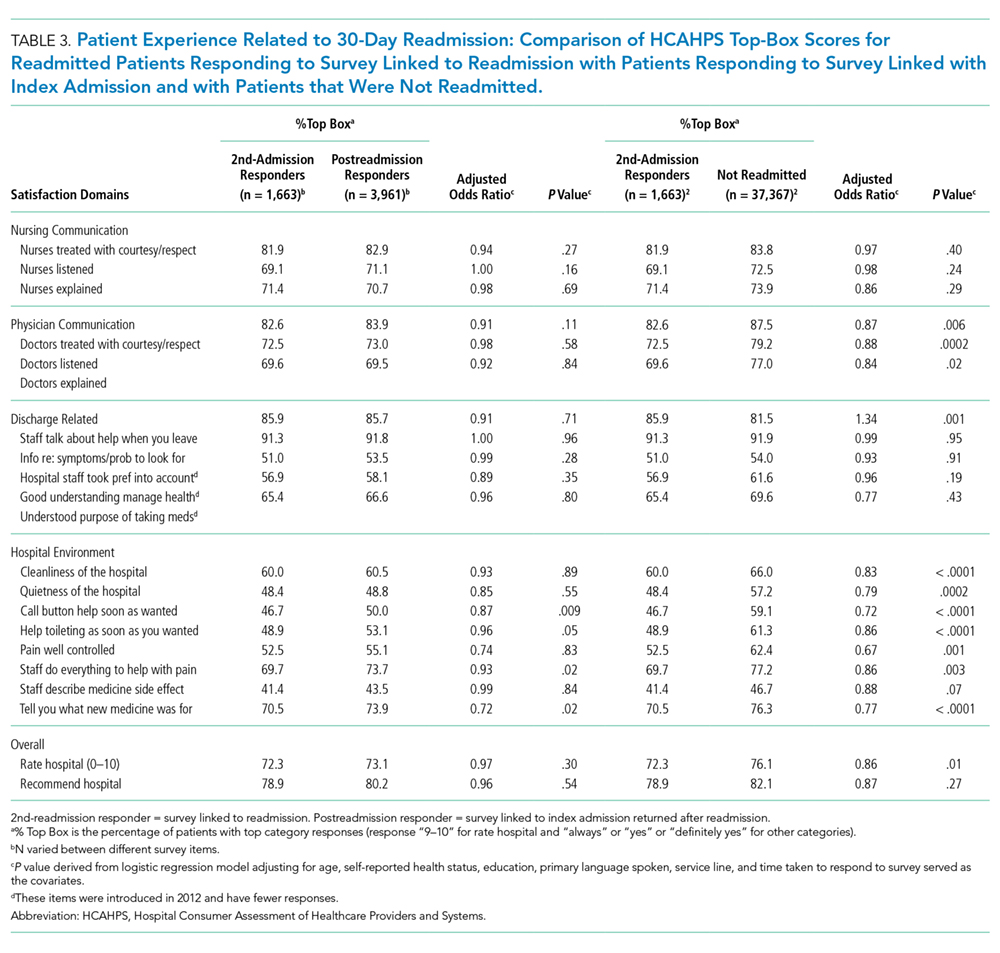
RESULTS: Only 15.8% of the readmitted patients responded to the survey prior to readmission, and their scores were not significantly different from the nonreadmitted patients. The patients who responded after readmission were significantly more dissatisfied with physicians (doctors listened 73.0% vs 79.2%, aOR 0.75, P < .0001), staff responsiveness, (call button 50.0% vs 59.1%, aOR 0.71, P < .0001) pain control, discharge plan, noise, and cleanliness of the hospital.
CONCLUSION: Our findings suggest that poor patient experience may be due to being readmitted, rather than being predictive of readmission.
© 2018 Society of Hospital Medicine
Statistical Analysis
“Percent top-box” scores were calculated for each survey item for patients in each group. The percent top-box scores were calculated as the percent of patients who responded “very good” for a given item on Press Ganey survey items and “always” or “definitely yes” or “yes” or “9” or “10” on HCAHPS survey items. CMS utilizes “percent top-box scores” to calculate payments under the VBP program and to report the results publicly. Numerous studies have also reported percent top-box scores for HCAHPS survey results.12
We hypothesized that whether patients complete the HCAHPS survey before or after the readmission influences their reporting of experience. To test this hypothesis, HCAHPS and Press Ganey item top-box scores of “Pre-readmission responders” and “Postreadmission responders” were compared with those of the control group using multivariate logistic regression. “Pre-readmission responders” were also compared with “Postreadmission responders”.
“2nd-admission responders” were similarly compared with the control group for an exploratory analysis. Finally, “Postreadmission responders” and “2nd-admission responders” were compared in another exploratory analysis since both these groups responded to the survey after being exposed to the readmission, even though the “Postreadmission responders” group is administratively linked to the index admission.
The Johns Hopkins Institutional Review Board approved this study.
RESULTS
There were 43,737 survey responders, among whom 4,707 were subsequently readmitted within 30 days of discharge. Among the readmitted patients who responded to the surveys linked to their index admission, only 15.8% returned the survey before readmission (pre-readmission responders’) and 84.2% returned the survey after readmission (postreadmission responders). Additionally, 1,663 patients responded to experience surveys linked to their readmission. There were 37,365 patients in the control arm (ie, patients who responded to the survey and were not readmitted within 30 days of discharge or in the prior 30 days; Figure 1). The readmission rate among survey responders was 10.6%. Among the readmitted patients, the median number of days to readmission was 10 days while the median number of days to respond to the survey for this group was 33 days. Among the nonreadmitted patients, the median number of days to return the survey was 29 days.

We also conducted an exploratory analysis of the postreadmission responders, comparing them with patients who received patient-experience surveys linked to their second admission in 30 days. Both of these groups were exposed to a readmission before they completed the surveys. There were no significant differences between these two groups on patient experience scores. Additionally, the patients who received the survey linked to their readmission had a broad dissatisfaction pattern on HCAHPS survey items that appeared similar to that of the postreadmission group when compared to the non-readmitted group (Table 3).