Improving Teamwork and Patient Outcomes with Daily Structured Interdisciplinary Bedside Rounds: A Multimethod Evaluation





BACKGROUND: Previous research has shown that interdisciplinary ward rounds have the potential to improve team functioning and patient outcomes.
DESIGN: A convergent parallel multimethod approach to evaluate a hospital interdisciplinary ward round intervention and ward restructure.
SETTING: An acute medical unit in a large tertiary care hospital in regional Australia.
PARTICIPANTS: Thirty-two clinicians and inpatients aged 15 years and above, with acute episode of care, discharged during the year prior and the year of the intervention.
INTERVENTION: A daily structured interdisciplinary bedside round combined with a ward restructure.
MEASUREMENTS: Qualitative measures included contextual factors and measures of change and experiences of clinicians. Quantitative measures included length of stay (LOS), monthly “calls for clinical review,’” and cost of care delivery.
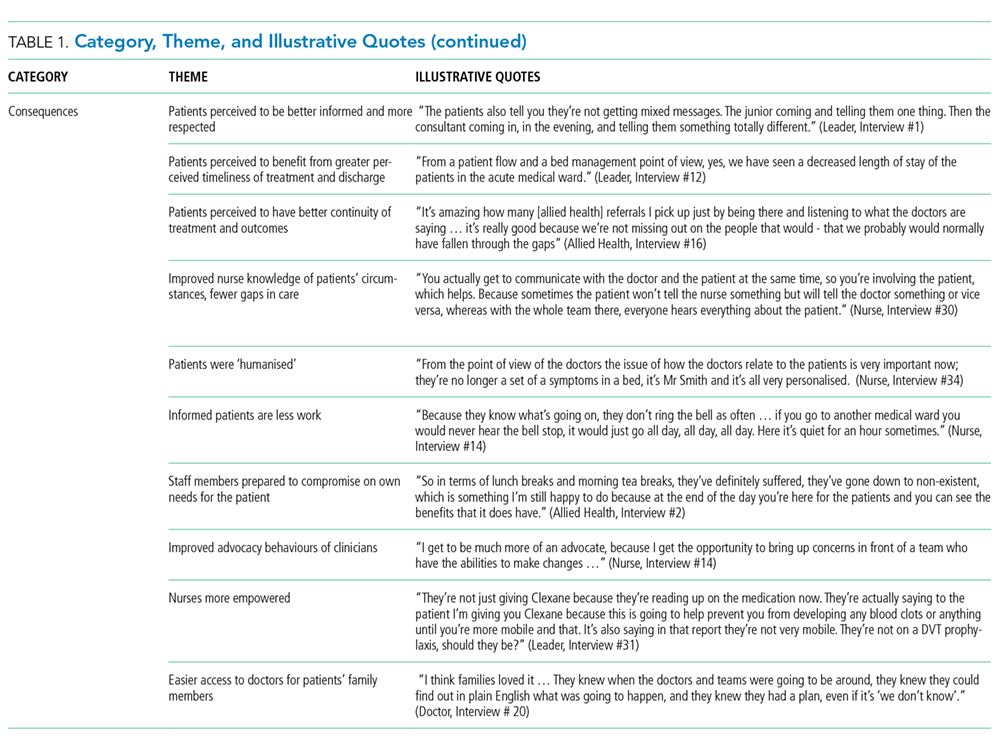
RESULTS: Clinicians reported improved teamwork, communication, and understanding between and within the clinical professions, and between clinicians and patients, after the intervention implementation. There was no statistically significant difference between the intervention and control wards in the change in LOS over time (Wald χ2 = 1.05; degrees of freedom [df] = 1; P = .31), but a statistically significant interaction for cost of stay, with a drop in cost over time, was observed in the intervention group, and an increase was observed in the control wards (Wald χ2 = 6.34; df = 1; P = .012). The medical wards and control wards differed significantly in how the number of monthly “calls for clinical review” changed from prestructured interdisciplinary bedside round (SIBR) to during SIBR (F (1,44) = 12.18; P = .001).
CONCLUSIONS: Multimethod evaluations are necessary to provide insight into the contextual factors that contribute to a successful intervention and improved clinical outcomes.
© 2018 Society of Hospital Medicine
Themes
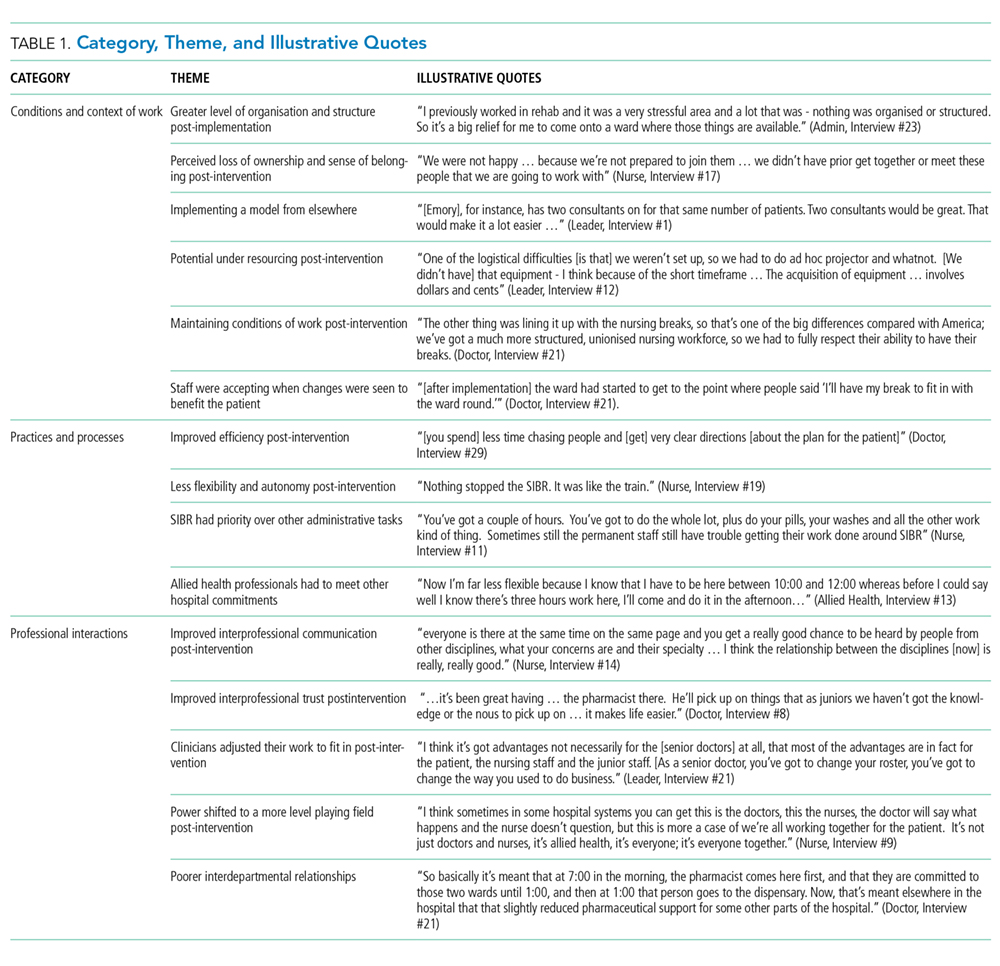
Context and Conditions of Work
Practices and Processes
Participants perceived postintervention work processes to be more efficient. A primary example was a near-universal approval of the time saved from not “chasing” other professionals now that they were predictably available on the ward. More timely decision-making was thought to result from this predicted availability and associated improvements in communication.
The SIBR enforced a workflow on all staff, who felt there was less flexibility to work autonomously (doctors) or according to patients’ needs (nurses). More junior staff expressed anxiety about delayed completion of discharge-related administrative tasks because of the midday completion of the round. Allied health professionals who had commitments in other areas of the hospital often faced a dilemma about how to prioritize SIBR attendance and activities on other wards. This was managed differently depending on the specific allied health profession and the individuals within that profession.
Professional Interactions
In terms of interprofessional dynamics on the AMU, the implementation of SIBR resulted in a shift in power between the doctors and the nurses. In the old ward, doctors largely controlled the timing of medical rounding processes. In the new AMU, doctors had to relinquish some control over the timing of personal workflow to comply with the requirements of SIBR. Furthermore, there was evidence that this had some impact on traditional hierarchical models of communication and created a more level playing field, as nonmedical professionals felt more empowered to voice their thoughts during and outside of rounds.
The rounds provided much greater visibility of the “big picture” and each profession’s role within it; this allowed each clinician to adjust their work to fit in and take account of others. The process was not instantaneous, and trust developed over a period of weeks. Better communication meant fewer misunderstandings, and workload dropped.
The participation of allied health professionals in the round enhanced clinician interprofessional skills and knowledge. The more inclusive approach facilitated greater trust between clinical disciplines and a development of increased confidence among nursing, allied health, and administrative professionals.
In contrast to the positive impacts of the new model of care on communication and relationships within the AMU, interdepartmental relationships were seen to have suffered. The processes and practices of the new AMU are different to those in the other hospital departments, resulting in some isolation of the unit and difficulties interacting with other areas of the hospital. For example, the trade-offs that allied health professionals made to participate in SIBR often came at the expense of other units or departments.
