Impact of a Multicenter, Mentored Quality Collaborative on Hospital-Associated Venous Thromboembolism





BACKGROUND: Reliable prophylaxis of hospital-associated venous thromboembolism (HA-VTE) is not achieved in many hospitals. Efforts to improve prophylaxis have had uneven results.
OBJECTIVE: To reduce HA-VTE with a scalable quality improvement collaborative.
DESIGN: A prospective, unblinded, open-intervention study with historical controls.
PARTICIPANTS AND SETTING: All adult inpatients at 35 community hospitals in California, Arizona, and Nevada.
INTERVENTIONS: A centrally supported collaborative implementing standardized VTE risk assessment and prophylaxis. Protocols were developed with 9 “pilot” sites, which received individualized mentoring. Finished protocols were disseminated to 26 “spread” sites, which received improvement webinars without mentoring. Active surveillance for real-time correction of suboptimal prophylaxis was funded in pilot sites and encouraged in spread sites. Planning and minimal improvement work began in 2011; most implementation occurred in 2012 and 2013.
MEASUREMENTS: Rates of per-protocol prophylaxis (at pilot sites), and compliance with The Joint Commission VTE measures (all sites), were monitored starting in January 2012. The International Classification of Diseases, 9th Edition-Clinical Modification codes were used to determine the rates of HA-VTE within 30 days of discharge, heparin-induced thrombocytopenia, and anticoagulation adverse events; preimplementation (2011) rates were compared with postimplementation (2014) rates.
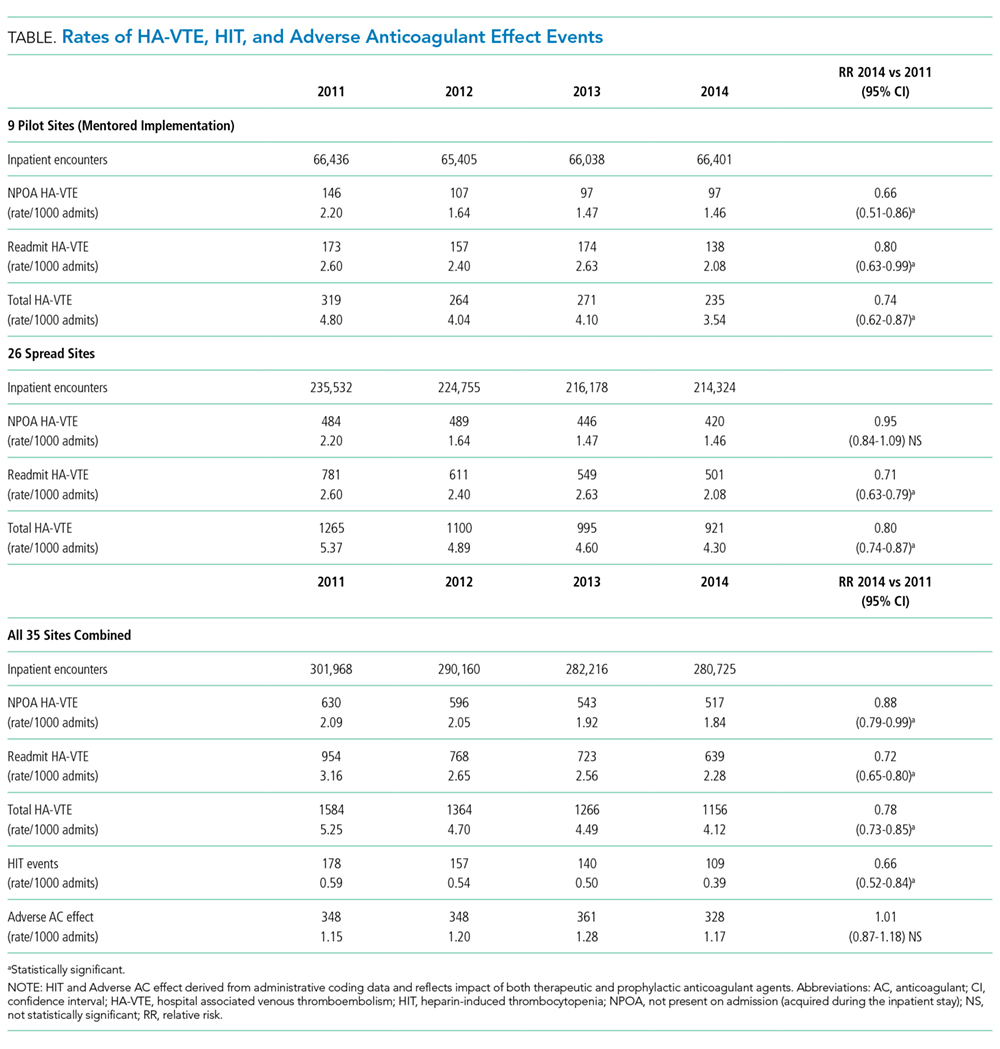
RESULTS: Protocol-appropriate prophylaxis rates and The Joint Commission measure compliance both reached 97% in 2014, up from 70% to 89% in 2012 and 2013. Five thousand three hundred and seventy HA-VTEs occurred during 1.16 million admissions. Four hundred twenty-eight fewer HA-VTEs occurred in 2014 than in 2011 (relative risk 0.78; 95% confidence interval, 0.73-0.85). HA-VTEs fell more in pilot sites than spread sites (26% vs 20%). The rates of adverse events were reduced or unchanged.
CONCLUSIONS: Collaborative efforts were associated with improved prophylaxis rates and fewer HA-VTEs.
© 2018 Society of Hospital Medicine
HA-VTE Rates
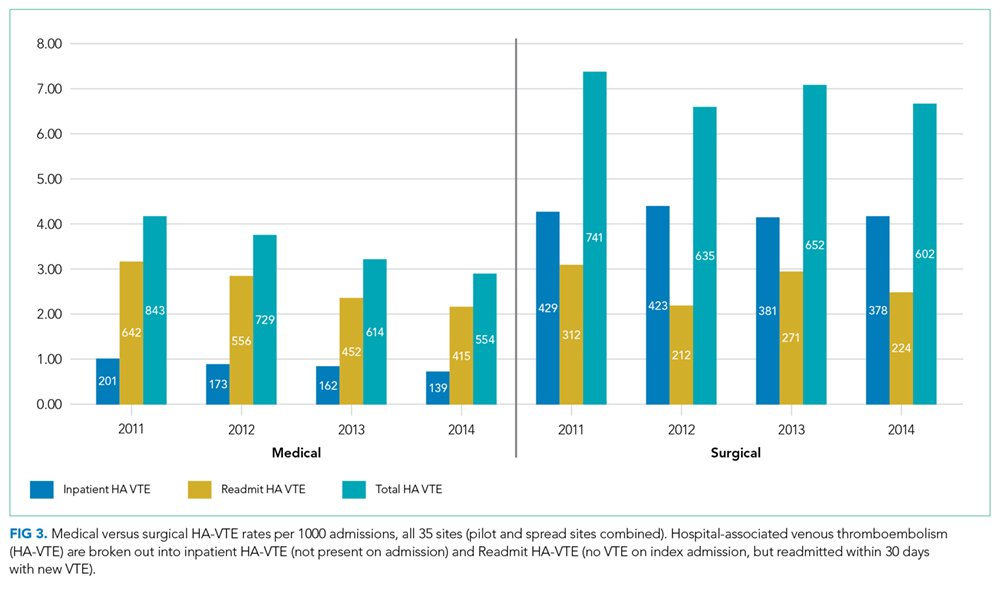
VTE events were captured by review of electronic coding data for the International Classification of Diseases, 9th Revision (ICD-9) codes 415.11-415.19, 453.2, 453.40-453.42, and 453.8-453.89. HA-VTE was defined as either new VTE not present on admission (NPOA HA-VTE) or new VTE presenting in a readmitted patient within 30 days of discharge (Readmit HA-VTE). Cases were stratified based on whether the patient had undergone a major operation (surgery patients) or not (medical patients) as identified by Medicare Services diagnosis-related group codes.
Control Measures
Potential adverse events were captured by review of electronic coding data for ICD-9 codes 289.84 (heparin-induced thrombocytopenia [HIT]) and E934.2 (adverse effects because of anticoagulants).
Statistical Analysis
Statistical process control charts were used to depict changes in prophylaxis rates over the 3 years for which data was collected. For VTE and safety outcomes, Pearson χ2 value with relative risk (RR) calculations and 95% confidence intervals (CIs) were used to compare proportions between groups at baseline (CY 2011) versus postimplementation (CY 2014). Differences between the means of normally distributed data were calculated, and a 95% CI for the difference between the means was performed to assess statistical difference. Nonparametric characteristics were described by quartiles and interquartile range, and the 2-sided Mann-Whitney U test was performed to assess statistical difference between the CY 2011 and CY 2014 period.
Role of the Funding Source
The GBMF funded the collaborative and supported authorship of the manuscript but had no role in the design or conduct of the intervention, the collection or analysis of data, or the drafting of the manuscript.
RESULTS
Population Demographics
There were 1,155,069 adult inpatient admissions during the 4-year study period (264,280 in the 9 pilot sites, 890,789 in the 26 spread sites). There were no clinically relevant changes in gender distribution, mortality rate, median age, case mix index, or hospital length of stay in 2011 versus 2014. Men comprised 47.1% of the patient population in 2011 and 47.7% in 2014. The mortality rate was 2.7% in both years. Median age was 62 in 2011 and 63 in 2014. The mean case mix index (1.58 vs 1.65) and mean length of stay (4.29 vs 4.33 days) were similar in the 2 time periods.
Prophylaxis Rates
TJC Prophylaxis rates

Rates of Protocol-Compliant Prophylaxis
There were 34,071 active surveillance audits across the 20 months of reporting in the pilot cohort (mean, 1817 audits per month). The rate of protocol-compliant prophylaxis improved from 89% at month 1 of observation to 93% during month 2 and 97% by the last 3 months (Pearson χ2 P < .001 for both comparisons).
HA-VTE
HA-VTE characteristics
Improved HA-VTE over Time
Four hundred twenty-eight fewer HA-VTEs occurred in 2014 than in 2011 (RR 0.78; 95% CI, 0.73-0.85) (Table and Figure 3). Readmission HA-VTEs were reduced by 315 (RR 0.72; 95% CI, 0.65-0.80), while the reduction in NPOA HA-VTEs was less robust (RR 0.88; 95% CI, 0.79-0.99). Pilot sites enjoyed a more robust reduction in HA-VTEs than spread sites (26% vs 20%), largely because the pilot cohort enjoyed a 34% reduction in NPOA HA-VTEs and a 20% reduction in Readmit HA-VTEs, while the spread cohort only achieved reductions in Readmit HA-VTEs.