Patterns and Predictors of Short-Term Peripherally Inserted Central Catheter Use: A Multicenter Prospective Cohort Study





BACKGROUND: The guidelines for peripherally inserted central catheters (PICCs) recommend avoiding insertion if the anticipated duration of use is ≤5 days. However, short-term PICC use is common in hospitals. We sought to identify patient, provider, and device characteristics and the clinical outcomes associated with short-term PICCs.
METHODS: Between January 2014 and June 2016, trained abstractors at 52 Michigan Hospital Medicine Safety (HMS) Consortium sites collected data from medical records of adults that received PICCs during hospitalization. Patients were prospectively followed until PICC removal, death, or 70 days after insertion. Multivariable logistic regression models were fit to identify factors associated with short-term PICCs, defined as dwell time of ≤5 days. Complications associated with short-term use, including major (eg, venous thromboembolism [VTE] or central line-associated bloodstream infection [CLABSI]) or minor (eg, catheter occlusion, tip migration) events were assessed.
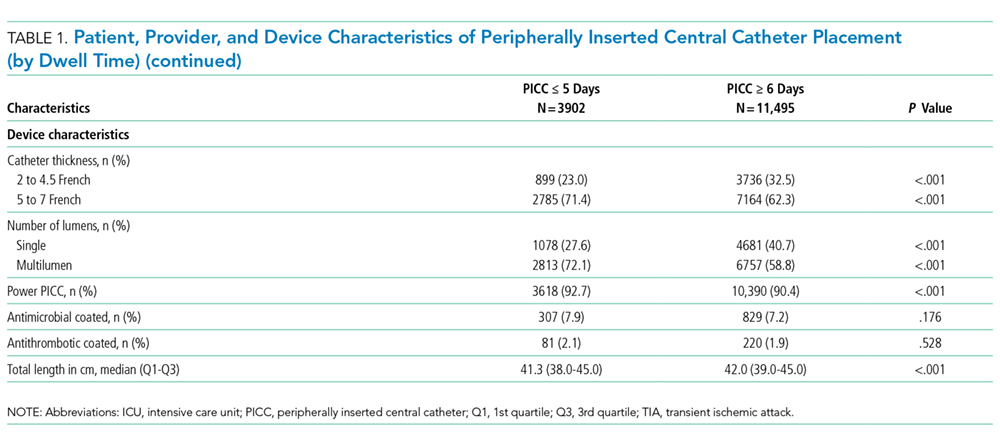
RESULTS: Of the 15,397 PICCs placed, 3902 (25.3%) had a dwell time of ≤5 days. Most (95.5%) short-term PICCs were removed during hospitalization. Compared to PICCs placed for >5 days, variables associated with short-term PICCs included difficult venous access (odds ratio [OR], 1.54; 95% confidence interval [CI], 1.40-1.69), multilumen devices (OR, 1.53; 95% CI, 1.39-1.69), and teaching hospitals (OR, 1.25; 95% CI, 1.04-1.52). Among those with short-term PICCs, 374 (9.6%) experienced a complication, including 99 (2.5%) experiencing VTE and 17 (0.4%) experiencing CLABSI events. The most common minor complications were catheter occlusion (4%) and tip migration (2.2%).
CONCLUSION: Short-term use of PICCs is common and associated with patient, provider, and device factors. As PICC placement, even for brief periods, is associated with complications, efforts targeted at factors underlying such use appear necessary.
© 2018 Society of Hospital Medicine
Patient, Provider, and Device Data
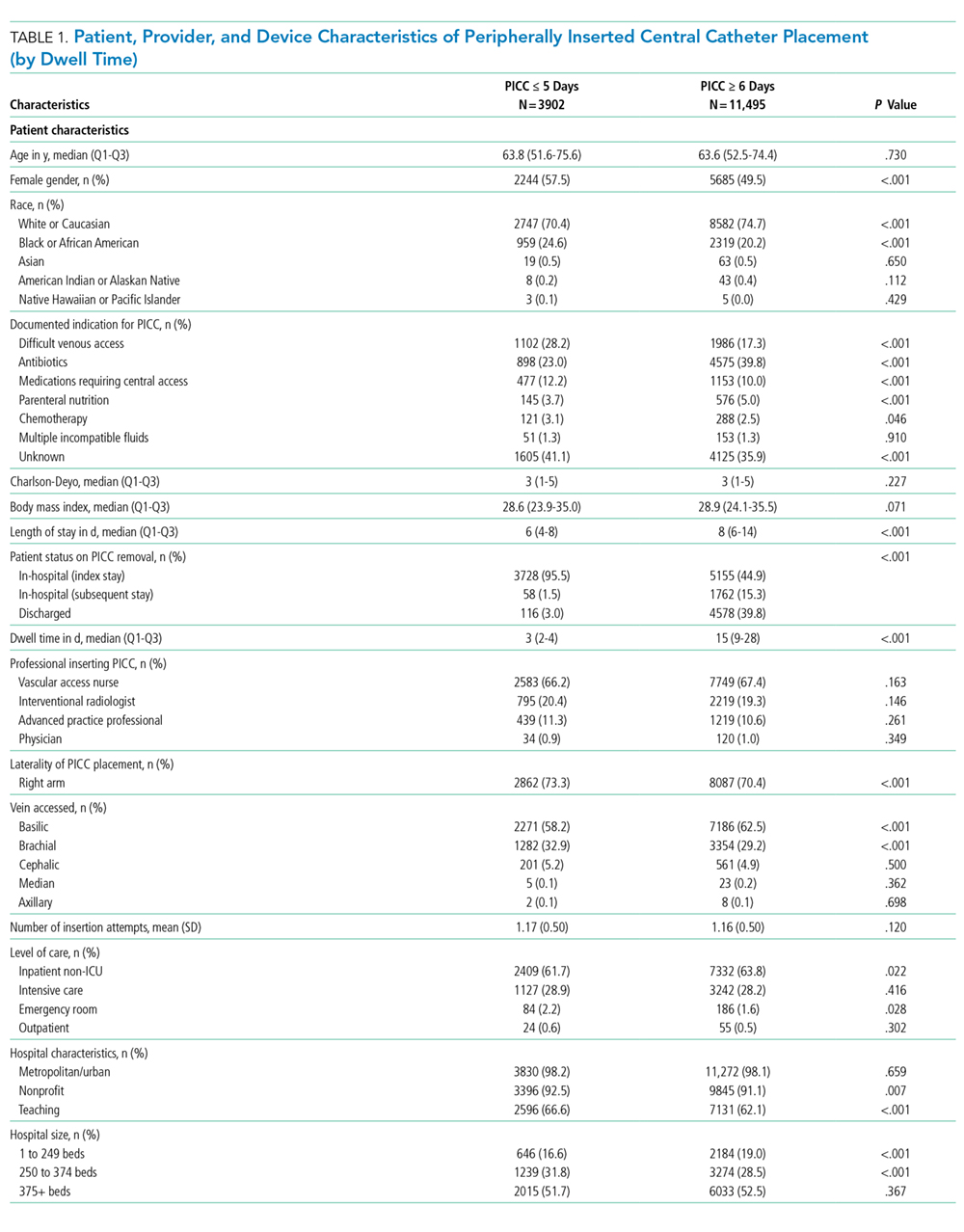
Patient characteristics, including demographics, detailed medical history, comorbidities, physical findings, laboratory results, and medications were abstracted directly from medical records. To estimate the comorbidity burden, the Charlson-Deyo comorbidity score was calculated for each patient by using data available in the medical record at the time of PICC placement.18 Data, such as the documented indication for PICC insertion and the reason for removal, were obtained directly from medical records. Provider characteristics, including the specialty of the attending physician at the time of insertion and the type of operator who inserted the PICC, were also collected. Institutional characteristics, such as total number of beds, teaching versus nonteaching, and urban versus rural, were obtained from hospital publicly reported data and semiannual surveys of HMS sites.19,20 Data on device characteristics, such as catheter gauge, coating, insertion attempts, tip location, and number of lumens, were abstracted from PICC insertion notes.
Outcomes of Interest
The outcome of interest was short-term PICC use, defined as PICCs removed within 5 days of insertion. Patients who expired with a PICC in situ were excluded. Secondary outcomes of interest included PICC-related complications, categorized as major (eg, symptomatic VTE and CLABSI) or minor (eg, catheter occlusion, superficial thrombosis, mechanical complications [kinking, coiling], exit site infection, and tip migration). Symptomatic VTE was defined as clinically diagnosed deep venous thrombosis (DVT) and/or pulmonary embolism (PE) not present at the time of PICC placement and confirmed via imaging (ultrasound or venogram for DVT; computed tomography scan, ventilation perfusion scan, or pulmonary angiogram for PE). CLABSI was defined in accordance with the CDC’s National Healthcare Safety Network criteria or according to Infectious Diseases Society of America recommendations.21,22 All minor PICC complications were defined in accordance with prior published definitions.4
Statistical Analysis
Cases of short-term PICC use were identified and compared with patients with a PICC dwell time of 6 or more days by patient, provider, and device characteristics. The initial analyses for the associations of putative factors with short-term PICC use were performed using χ2 or Wilcoxon tests for categorical and continuous variables, respectively. Univariable mixed effect logistic regression models (with a random hospital-specific intercept) were then used to control for hospital-level clustering. Next, a mixed effects multivariable logistic regression model was used to identify factors associated with short-term PICC use. Variables with P ≤ .25 were considered as candidate predictors for the final multivariable model, which was chosen through a stepwise variable selection algorithm performed on 1000 bootstrapped data sets.23 Variables in the final model were retained based on their frequency of selection in the bootstrapped samples, significance level, and contribution to the overall model likelihood. Results were expressed as odds ratios (OR) with corresponding 95% confidence intervals (CI). SAS for Windows (version 9.3, SAS Institute Inc., Cary, NC) was used for analyses.
Ethical and Regulatory Oversight
The study was classified as “not regulated” by the Institutional Review Board at the University of Michigan (HUM00078730).
RESULTS
Overall Characteristics of the Study Cohort
Characteristics of Short-Term Peripherally Inserted Central Catheter Use
Of the 15,397 PICCs included, we identified 3902 PICCs (25.3%) with a dwell time of ≤5 days (median = 3 days; IQR, 2-4 days). When compared to PICCs that were in place for longer durations, no significant differences in age or comorbidity scores were observed. Importantly, despite recommendations to avoid PICCs in patients with moderate to severe chronic kidney disease (glomerular filtration rate [GFR] ≤ 59 ml/min), 1292 (33.1%) short-term PICCs occurred in patients that met such criteria.