Hospital Perceptions of Medicare’s Sepsis Quality Reporting Initiative





BACKGROUND: In October 2015, the Centers for Medicare and Medicaid Services (CMS) implemented the Sepsis CMS Core Measure (SEP-1) program, requiring hospitals to report data on the quality of care for their patients with sepsis.
OBJECTIVE: We sought to understand hospital perceptions of and responses to the SEP-1 program.
DESIGN: A thematic content analysis of semistructured interviews with hospital quality officials.
SETTING: A stratified random sample of short-stay, nonfederal, general acute care hospitals in the United States.
SUBJECTS: Hospital quality officers, including nurses and physicians.
INTERVENTION: None.
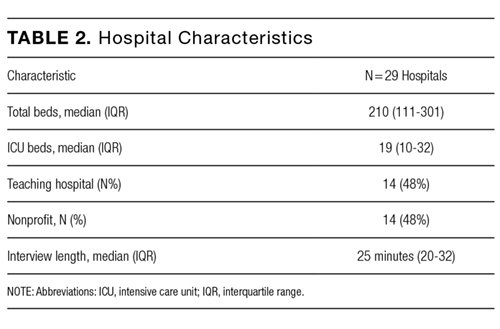
MEASUREMENTS: We completed 29 interviews before reaching content saturation.
RESULTS: Hospitals reported a variety of actions in response to SEP-1, including new efforts to collect data, improve sepsis diagnosis and treatment, and manage clinicians’ attitudes toward SEP-1. These efforts frequently required dedicated resources to meet the program’s requirements for treatment and documentation, which were thought to be complex and not consistently linked to patient-centered outcomes. Most respondents felt that SEP-1 was likely to improve sepsis outcomes. At the same time, they described specific changes that could improve its effectiveness, including allowing hospitals to focus on the treatment processes most directly associated with improved patient outcomes and better aligning the measure’s sepsis definitions with current clinical definitions.
CONCLUSIONS: Hospitals are responding to the SEP-1 program across a number of domains and in ways that consistently require dedicated resources. Hospitals are interested in further revisions to the program to alleviate the burden of the reporting requirements and help them optimize the effectiveness of their investments in quality-improvement efforts.
© 2017 Society of Hospital Medicine
Analysis
Interviews were audio recorded, transcribed, and loaded onto a secure server. We used NVivo 11 (QSR International, Cambridge, Massachusetts) for coding and analysis. We iteratively reviewed and thematically analyzed the transcripts for structural content and emergent themes, consistent with established qualitative methods.15 Three investigators reviewed the initial 20 transcripts and developed the codebook through iterative discussion and consensus. The codes were then organized into themes and subthemes. Subsequently, 1 investigator coded the remaining transcripts. The results are presented as a series of key themes supported by direct quotes from the interviews.
RESULTS
Sample Description
Perspectives on SEP-1

Responses to SEP-1

Efforts to Collect Data for SEP-1 Reporting
Respondents reported challenges in reliably and validly measuring and reporting data for the SEP-1 program. First, patient identification and the measurement of treatment processes depends largely on manual medical record review, which is subject to variation across coders. This presents a particular challenge because the clinical definition of sepsis itself is in evolution,1 creating the possibility that treating physicians could identify a given patient as having sepsis or septic shock based on the most up-to-date definitions but not based on the measure’s specifications or vice versa. Second, each case requires up to an hour of manual medical record review and patients who develop sepsis during prolonged hospitalizations can require several hours or more, which is an unprecedented length of time to spend abstracting data for a single measure.
In addressing these measurement challenges, investment in human resources is the rule. No respondent reported automating abstraction of all the SEP-1 data elements, underscoring concerns regarding the measurement burden of the SEP-1 program.7,8,14 Rather, hospitals with sufficient financial resources frequently employ full-time data abstractors and individuals responsible for ongoing performance feedback, which facilitates the iterative revision of sepsis quality-improvement initiatives. In contrast, hospitals with fewer resources often rely on contracts with third-party vendors, which delays reporting and complicates efforts to use the data for individualized performance improvement.
Efforts to Coordinate Hospital Responses Across Care Teams
Complying with the measure involves the longitudinal coordination of multiple care teams across different units, so planning and executing local hospital responses required interdepartmental and multidisciplinary stakeholder involvement. Respondents were uncertain about the ideal strategy to coordinate these quality-improvement efforts, yielding iterative changes to electronic health records (EHRs), education programs, and data collection methods. This “learning by doing” is necessary because no prior CMS quality measure is as complex as SEP-1 or as varied in the sources of data required to measure and report the results. By requiring hospitals to improve coordination of care throughout the hospital, SEP-1 presents a quality-improvement and measurement challenge that may ultimately drive innovation and better patient care.