The Effect of an Inpatient Smoking Cessation Treatment Program on Hospital Readmissions and Length of Stay





BACKGROUND: Most clinical research involving tobacco dependence treatment is related to outpatient interventions and focuses on health outcomes. Inpatient smoking cessation treatment has been found to be cost-effective in the Canadian healthcare system, but the finding’s applicability to US health systems is unclear.
OBJECTIVE: The objective of this study is to estimate the impact of an inpatient tobacco cessation treatment program on 30-day readmission rates and length of stay (LOS).
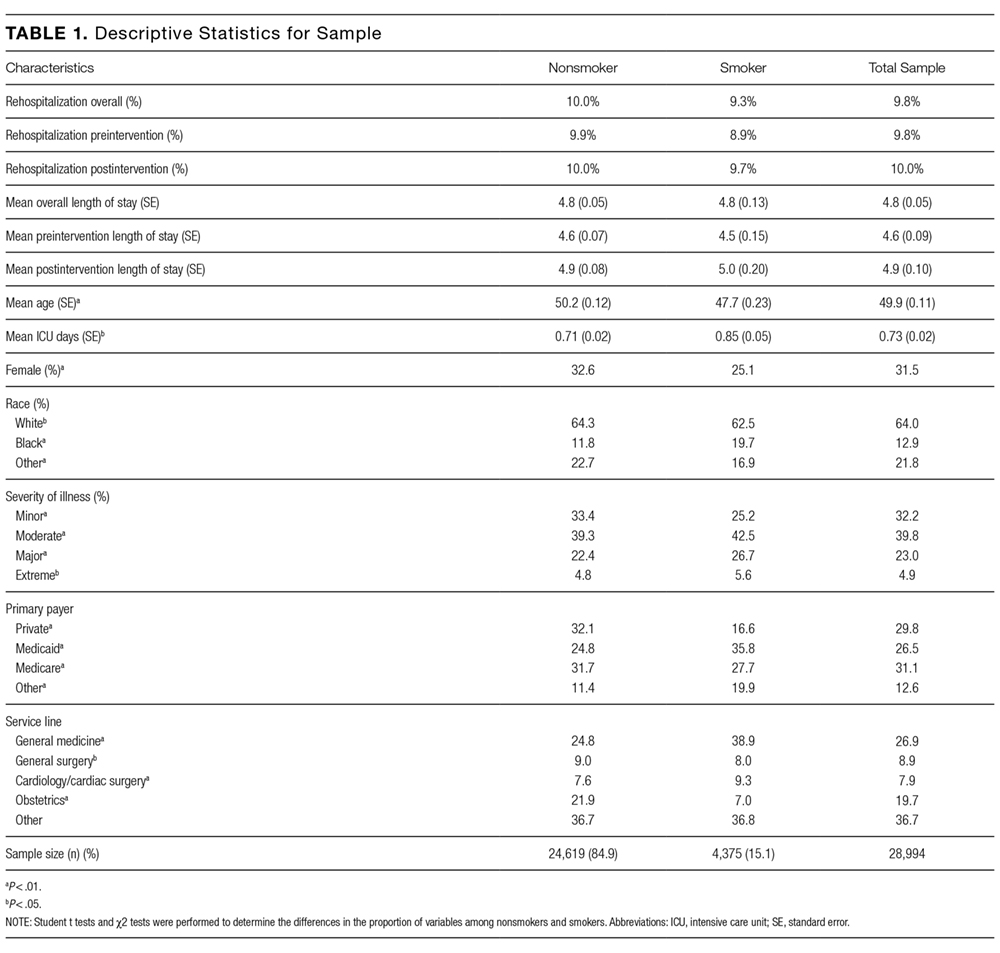
METHODS: Participants were 28,994 patients admitted to the hospital between July 2012 and July 2014. Smokers were identified through the electronic medical records system and were offered cessation treatment. Program effects were estimated by using a difference-in-differences approach, comparing all smokers to all nonsmokers before versus after introduction of the program. Readmission rates were modeled by using probit regression; LOS was modeled by using truncated negative binomial regression. Models controlled for age, sex, race, payer, hospital department, severity of illness, and intensive care unit days.
RESULTS: The hospital-initiated smoking cessation intervention had no significant effect on 30-day readmission rates or LOS. Other control variables had the expected signs and were statistically significant.
CONCLUSIONS: The evaluation of an inpatient tobacco dependence treatment did not find significant short-term changes in healthcare utilization in the first 30 days after initial hospitalization.
© 2017 Society of Hospital Medicine
Statistical Analysis
We used an intent-to-treat (ITT) framework for the analysis, which considers everyone eligible for the treatment to be in the treatment group. The approach ignores treatment nonacceptance, nonadherence, protocol deviations, withdrawal from treatment, and cessation outcomes,
Readmission rates and LOS were estimated by using a “difference-in-differences” model, comparing outcomes between smokers before versus after the introduction of the cessation treatment program with nonsmokers before versus after program introduction. The difference-in-differences method looks at the difference pre-and-post in the exposed group (smokers) and unexposed group (nonsmokers). Subtracting the difference between the 2 groups gives an estimate of the policy effect controlling for background trends.19 The smoking cessation treatment effect on readmission is measured by the coefficient on the interaction term between the smoking variable and an indicator that the program is operational. The coefficient is the “difference-in-differences.”
Other control variables include demographic factors (gender, age, race), hospitalization payer (Medicare, Medicaid, commercial), and the service line of the admission. We also included a severity of illness variable from the APR-DRG Grouper (3M, Maplewood, Minnesota)20 and the number of days spent in the intensive care unit. For the readmission model, we included LOS as a control variable, because individuals with longer LOS had a better opportunity to access the intervention.
For readmissions, the model was estimated by using a probit model, predicting the effect of each of the intervention variables and the control variables on the marginal probability of a readmission. Because patients can appear in both the pre- and postyears, clustered standard errors were used, which correct for the lack of independence from multiple observations from the same individual.21 For LOS, a truncated negative binomial model was used. The negative binomial model is a specification for count models with a mass of observations plus a long right tail. The truncation is because zero and negative values for LOS are not possible. The dependent variable represents the number of days the individual was hospitalized. For both models, the reported coefficients represent the marginal effect of the independent variable on the dependent variable. This was calculated using the “margins” command in Stata version 13 (StataCorp LLC, College Station, Texas).
RESULTS
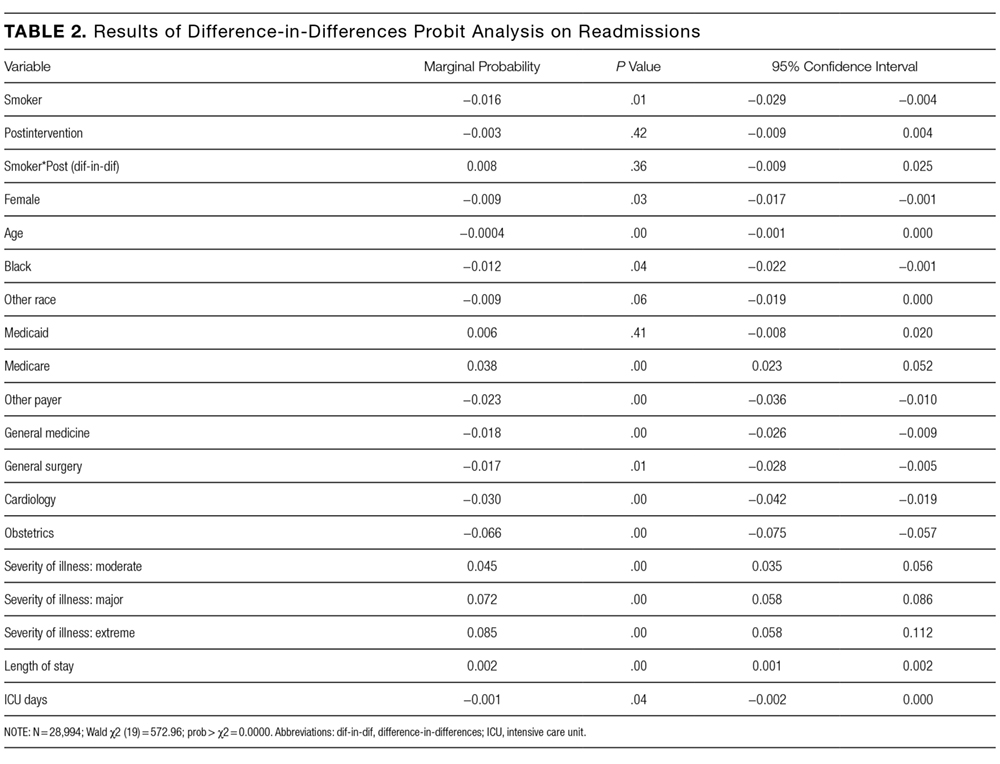
In the probit analysis, the smoking cessation intervention (Smoker*post intervention) showed no significant effect on the probability of readmission (Table 2). The coefficient is positive (β = 0.008) and statistically insignificant (P = 0.36). This indicates that we failed to reject the null hypothesis that there was not a systematic difference in the probability of readmission because of the smoking cessation intervention. Other significant variables generally had the expected relationship with readmission rates. Smokers were 1.6% less likely to be readmitted than nonsmokers (P = 0.01), controlling for other factors.
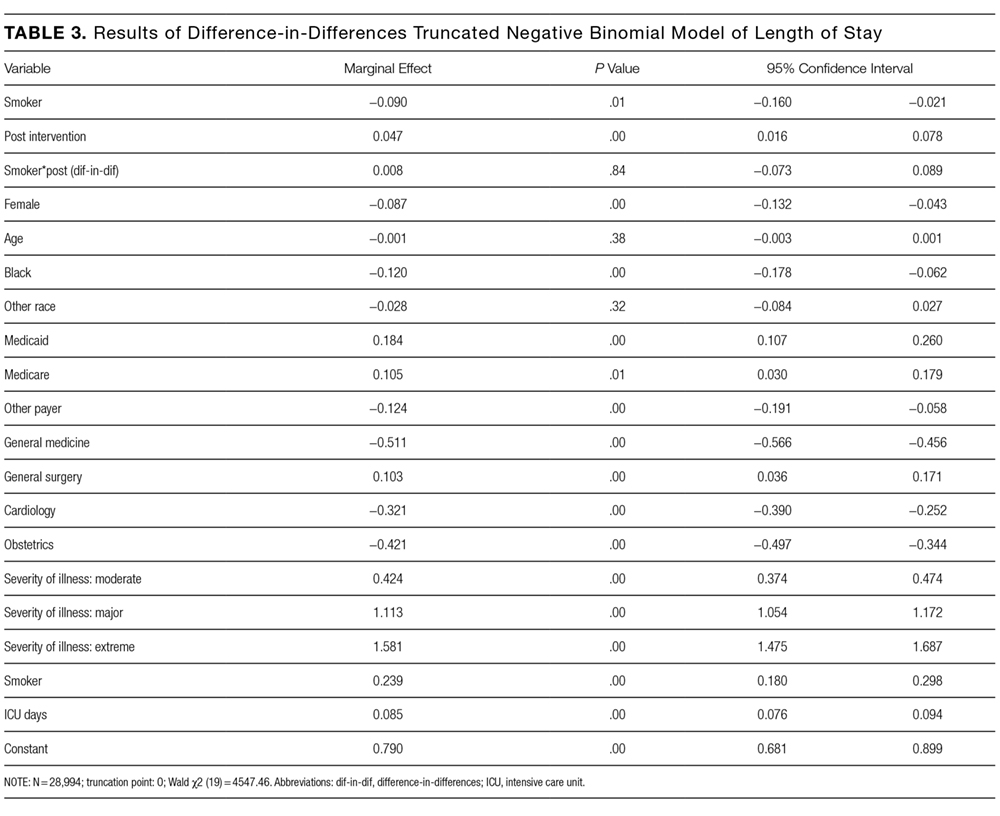
The program effect on smoker LOS was statistically insignificant (β = 0.008; P = 0.36). Smokers overall had a shorter LOS than nonsmokers (β = −0.090; P = 0.01), controlling for other factors. Overall LOS was longer postintervention (β = 0.047; P < 0.01). The control variables generally had the same relationship for the LOS model as for the readmission model.