Association Between Anemia and Fatigue in Hospitalized Patients: Does the Measure of Anemia Matter?





BACKGROUND: Restrictive blood transfusion practices in hospitalized patients with anemia have reduced the use of transfusion. Consequently, hospitalized patients are more likely to have lower hemoglobin (Hb) concentrations. Lower Hb is associated with increased fatigue in ambulatory patients. However, it is not known whether anemia is associated with fatigue in hospitalized patients. It is also unclear how to best measure anemia in hospitalized patients because Hb levels generally vary over a hospital stay.
OBJECTIVE: To assess multiple Hb-based measures of anemia in hospitalized patients and test whether these are associated with fatigue.
DESIGN: Prospective observational study.
SETTING: Urban, academic medical center.
PATIENTS: Hospitalized general medicine patients, age ≥50 years, with any Hb < 9 g/dL.
INTERVENTION: Patients’ anemia-related fatigue was measured during hospitalization.
MEASUREMENTS: Measures of anemia were created for each patient based on the Hb values from their hospitalization (mean, median, minimum, maximum, admission, and discharge). Fatigue was measured using the Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue subscale.
RESULTS: Seven hundred eighty-four patients participated. Minimum Hb was strongly associated with fatigue. Patients with a minimum Hb of < 8 g/dL had higher fatigue levels (mean FACIT [standard deviation] Hb < 7 g/dL: 25 [13], 7 g/dL ≤ Hb <8 g/dL: 25 [14] Hb ≥8 g/dL: 29 [14], P ≤ 0.001) and were more likely to report high levels of fatigue (FACIT-Fatigue < 27) (56% vs 41%; P = 0.002). Mean Hb had a less robust association with fatigue than minimum Hb, and no other measure of Hb was associated with patients’ fatigue levels.
CONCLUSION: Minimum Hb is associated with fatigue while hospitalized and may help identify patients for interventions to address anemia-related fatigue.
© 2017 Society of Hospital Medicine
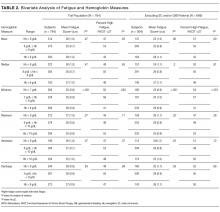
Linear Regression of Fatigue on Hb

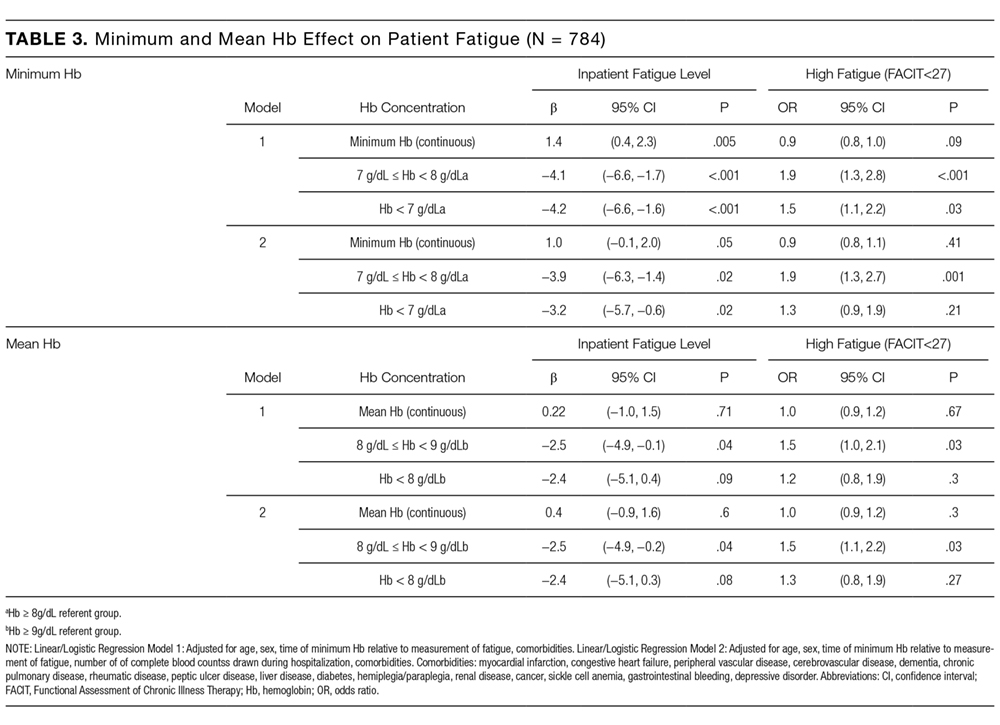
In linear regression models, minimum Hb consistently predicted patient fatigue, mean Hb had a less robust association with fatigue, and the other Hb measures were not associated with patient fatigue. Increases in minimum Hb (analyzed as a continuous variable) were associated with reduced fatigue (higher FACIT score; β = 1.4; P = 0.005). In models in which minimum Hb was a categorical variable, patients with a minimum Hb of <7 g/dL or 7-8 g/dL had greater fatigue (lower FACIT score) than patients whose minimum Hb was ≥8 g/dL (Hb <7 g/dL: β = −4.2; P ≤ 0.001; Hb 7-8 g/dL: β = −4.1; P < 0.001). These results control for patients’ age, sex, individual comorbidities, and whether their minimum Hb occurred before or after the measurement of fatigue during hospitalization (Model 1), and the results are unchanged when also controlling for the number of Hb laboratory draws patients had during their hospitalization (Model 2; Table 3). In a stratified analysis excluding patients with either SC and/or GIB, changes in minimum Hb were associated with larger changes in patient fatigue levels (Supplemental Table 1). We also stratified our analysis to include only patients whose minimum Hb occurred before the measurement of their fatigue level during hospitalization to avoid a spurious association of fatigue with minimum Hb occurring after fatigue was measured. In both Models 1 and 2, minimum Hb remained a predictor of patients’ fatigue levels with similar effect sizes, although in Model 2, the results did not quite reach a statistically significant level, in part due to larger confidence intervals from the smaller sample size of this stratified analysis (Supplemental Table 2a). We further stratified this analysis to include only patients whose transfusion, if they received one, occurred after their minimum Hb and the measurement of their fatigue level to account for the possibility that a transfusion could affect the fatigue level patients report. In this analysis, most of the estimates of the effect of minimum Hb on fatigue were larger than those seen when only analyzing patients whose minimum Hb occurred before the measurement of their fatigue level, although again, the smaller sample size of this additional stratified analysis does produce larger confidence intervals for these estimates (Supplemental Table 2b).
No Hb measure other than minimum or mean had significant association with patient fatigue levels in linear regression models.
Logistic Regression of High Fatigue Level on Hb
Using logistic regression, minimum Hb analyzed as a categorical variable predicted increased odds of a high fatigue level. Patients with a minimum Hb <7 g/dL were 50% (odds ratio [OR] = 1.5; P = 0.03) more likely to have high fatigue and patients with a minimum Hb 7-8 g/dL were 90% (OR = 1.9; P < 0.001) more likely to have high fatigue compared with patients with a minimum Hb ≥8 g/dL in Model 1. These results were similar in Model 2, although the effect was only statistically significant in the 7-8 g/dL Hb group (Table 3). When excluding SC and/or GIB patients, the odds of having high fatigue as minimum Hb decreased were the same or higher for both models compared to the full population of patients. However, again, in Model 2, the effect was only statistically significant in the 7-8 g/dL Hb group (Supplemental Table 1).
Patients with a mean Hb <8 g/dL were 20% to 30% more likely to have high fatigue and patients with mean Hb 8-9 g/dL were 50% more likely to have high fatigue compared with patients with a mean Hb ≥9 g/dL, but the effects were only statistically significant for patients with a mean Hb 8-9 g/dL in both Models 1 and 2 (Table 3). These results were similar when excluding patients with SC and/or GIB, but they were only significant for patients with a mean Hb 8-9 g/dL in Model 1 and patients with a mean Hb <8 g/dL in the Model 2 (Supplemental Table 3).
DISCUSSION
These results demonstrate that minimum Hb during hospitalization is associated with fatigue in hospitalized patients age ≥50 years, and the association is stronger among patients without SC and/or GIB as comorbidities. The analysis of Hb as a continuous and categorical variable and the use of both linear and logistic regression models support the robustness of these associations and illuminate their clinical significance. For example, in linear regression with minimum Hb a continuous variable, the coefficient of 1.4 suggests that an increase of 2 g/dL in Hb, as might be expected from transfusion of 2 units of red blood cells, would be associated with about a 3-point improvement in fatigue. Additionally, as a categorical variable, a minimum Hb ≥8 g/dL compared with a minimum Hb <7 g/dL or 7-8 g/dL is associated with a 3- to 4-point improvement in fatigue. Previous literature suggests that a difference of 3 in the FACIT score is the minimum clinically important difference in fatigue,3 and changes in minimum Hb in either model predict changes in fatigue that are in the range of potential clinical significance.
