Association Between Anemia and Fatigue in Hospitalized Patients: Does the Measure of Anemia Matter?





BACKGROUND: Restrictive blood transfusion practices in hospitalized patients with anemia have reduced the use of transfusion. Consequently, hospitalized patients are more likely to have lower hemoglobin (Hb) concentrations. Lower Hb is associated with increased fatigue in ambulatory patients. However, it is not known whether anemia is associated with fatigue in hospitalized patients. It is also unclear how to best measure anemia in hospitalized patients because Hb levels generally vary over a hospital stay.
OBJECTIVE: To assess multiple Hb-based measures of anemia in hospitalized patients and test whether these are associated with fatigue.
DESIGN: Prospective observational study.
SETTING: Urban, academic medical center.
PATIENTS: Hospitalized general medicine patients, age ≥50 years, with any Hb < 9 g/dL.
INTERVENTION: Patients’ anemia-related fatigue was measured during hospitalization.
MEASUREMENTS: Measures of anemia were created for each patient based on the Hb values from their hospitalization (mean, median, minimum, maximum, admission, and discharge). Fatigue was measured using the Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue subscale.
RESULTS: Seven hundred eighty-four patients participated. Minimum Hb was strongly associated with fatigue. Patients with a minimum Hb of < 8 g/dL had higher fatigue levels (mean FACIT [standard deviation] Hb < 7 g/dL: 25 [13], 7 g/dL ≤ Hb <8 g/dL: 25 [14] Hb ≥8 g/dL: 29 [14], P ≤ 0.001) and were more likely to report high levels of fatigue (FACIT-Fatigue < 27) (56% vs 41%; P = 0.002). Mean Hb had a less robust association with fatigue than minimum Hb, and no other measure of Hb was associated with patients’ fatigue levels.
CONCLUSION: Minimum Hb is associated with fatigue while hospitalized and may help identify patients for interventions to address anemia-related fatigue.
© 2017 Society of Hospital Medicine
Measuring Anemia
Hb measures were available only when hospital providers ordered them as part of routine practice. The first Hb concentration <9 g/dL during a patient’s hospitalization, which made them eligible for study participation, was obtained through manual review of the EHR. All additional Hb values during the patient’s hospitalization were obtained from the hospital’s administrative data mart. All Hb values collected for each patient during the hospitalization were used to calculate summary measures of Hb during the hospitalization, including the mean Hb, median Hb, minimum Hb, maximum Hb, admission (first recorded) Hb, and discharge (last recorded) Hb. Hb measures were analyzed both as a continuous variable and as a categorical variable created by dividing the continuous Hb measures into integer ranges of 3 groups of approximately the same size.
Measuring Fatigue
Our primary outcome was patients’ level of fatigue reported during hospitalization, measured using the Functional Assessment of Chronic Illness Therapy (FACIT)-Anemia questionnaire. Fatigue was measured using a 13-question fatigue subscale,1,2,25 which measures fatigue within the past 7 days. Scores on the fatigue subscale range from 0 to 52, with lower scores reflecting greater levels of fatigue. As soon as patients met the eligibility criteria for study participation during their hospitalization (age ≥50 years and Hb <9 g/dL), they were approached to answer the FACIT questions. Values for missing data in the fatigue subscale for individual subjects were filled in using a prorated score from their answered questions as long as >50% of the items in the fatigue subscale were answered, in accordance with recommendations for addressing missing data in the FACIT.26 Fatigue was analyzed as a continuous variable and as a dichotomous variable created by dividing the sample into high (FACIT <27) and low (FACIT ≥27) levels of fatigue based on the median FACIT score of the population. Previous literature has shown a FACIT fatigue subscale score between 23 and 26 to be associated with an Eastern Cooperative Oncology Group (ECOG)27 C Performance Status rating of 2 to 33 compared to scores ≥27.
Statistical Analysis
Statistical analysis was performed using Stata statistical software (StataCorp, College Station, TX). Descriptive statistics were used to characterize patient demographics. Analysis of variance was used to test for differences in the mean fatigue levels across Hb measures. χ2 tests were performed to test for associations between high fatigue levels and the Hb measures. Multivariable analysis, including both linear and logistic regression models, were used to test the association of Hb concentration and fatigue. P values <0.05 using a 2-tailed test were deemed statistically significant.
RESULTS
Patient Characteristics
During the study period, 8559 patients were admitted to the general medicine service. Of those, 5073 (59%) consented for participation in the Hospitalist Project, and 3670 (72%) completed the Hospitalist Project inpatient interview. Of these patients, 1292 (35%) had Hb <9 g/dL, and 784 (61%) were 50 years or older and completed the FACIT questionnaire.
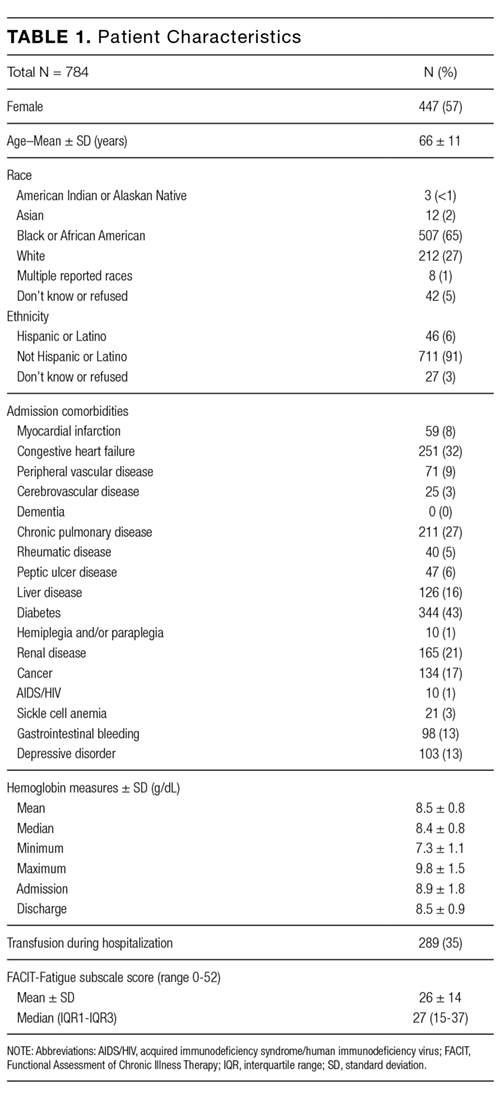
Table 1 reports the demographic characteristics and comorbidities for the sample, the mean (standard deviation [SD]) for the 6 Hb measures, and mean (SD) and median FACIT scores.
Bivariate Association of Fatigue and Hb
Categorizing patients into low, middle, or high Hb for each of the 6 Hb measures, minimum Hb was strongly associated with fatigue, with a weaker association for mean Hb and no statistically significant association for the other measures.
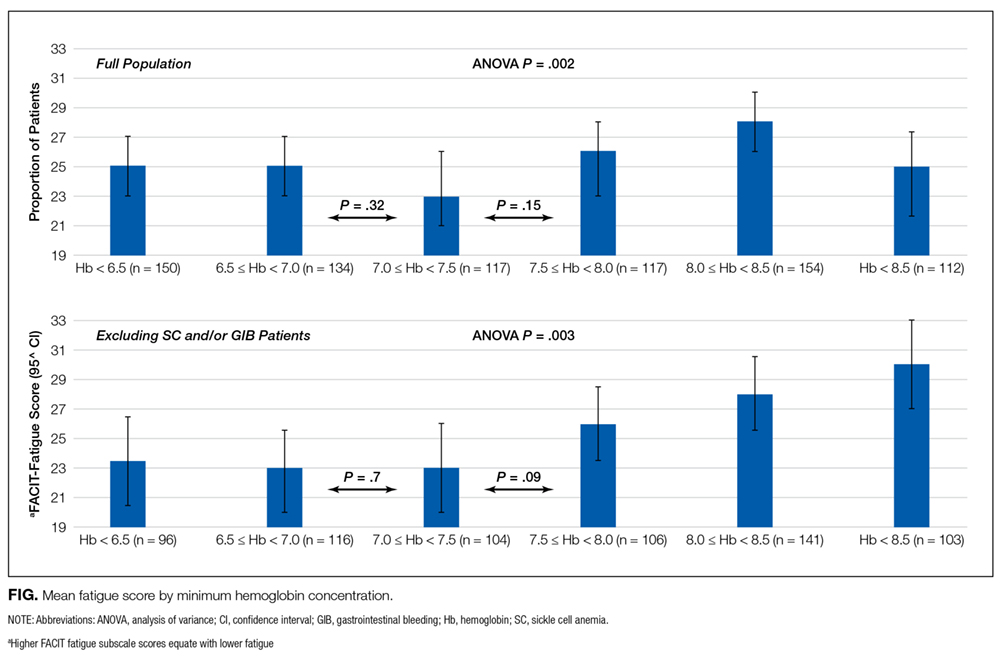
Minimum Hb. Patients with a minimum Hb <7 g/dL and patients with Hb 7-8 g/dL had higher fatigue levels (FACIT = 25 for each) than patients with a minimum Hb ≥8 g/dL (FACIT = 29; P < 0.001; Table 2). When excluding patients with SC and/or GIB because their average minimum Hb differed from the average minimum Hb of the full population (P < 0.001), patients with a minimum Hb <7 g/dL or 7-8 g/dL had even higher fatigue levels (FACIT = 23 and FACIT = 24, respectively), with no change in the fatigue level of patients with a minimum Hb ≥8 g/dL (FACIT = 29; P < 0.001; Table 2). Lower minimum Hb continued to be associated with higher fatigue levels when analyzed in 0.5 g/dL increments (Figure).
Mean Hb and Other Measures. Fatigue levels were high for 47% of patients with a mean Hb <8g /dL and 53% of patients with a mean Hb 8-9 g/dL compared with 43% of patients with a mean Hb ≥9 g/dL (P = 0.05). However, the association between high fatigue and mean Hb was not statistically significant when patients with SC and/or GIB were excluded (Table 2). None of the other 4 Hb measures was significantly associated with fatigue.
