Results
We had a 55.3% success rate in obtaining the medical records from the contacted hospitals with refusal to participate/consent by the hospital in question being the most frequent reason for failure in 3 out of 4 cases. An additional attrition of 39.3% was observed among the medical records received, with absence of a MAR form (23.9%) and confirmatory CDAD diagnosis or note (9.1%) being the most frequent criteria for discarding an available record prior to abstraction (Figure).
Patient Characteristics
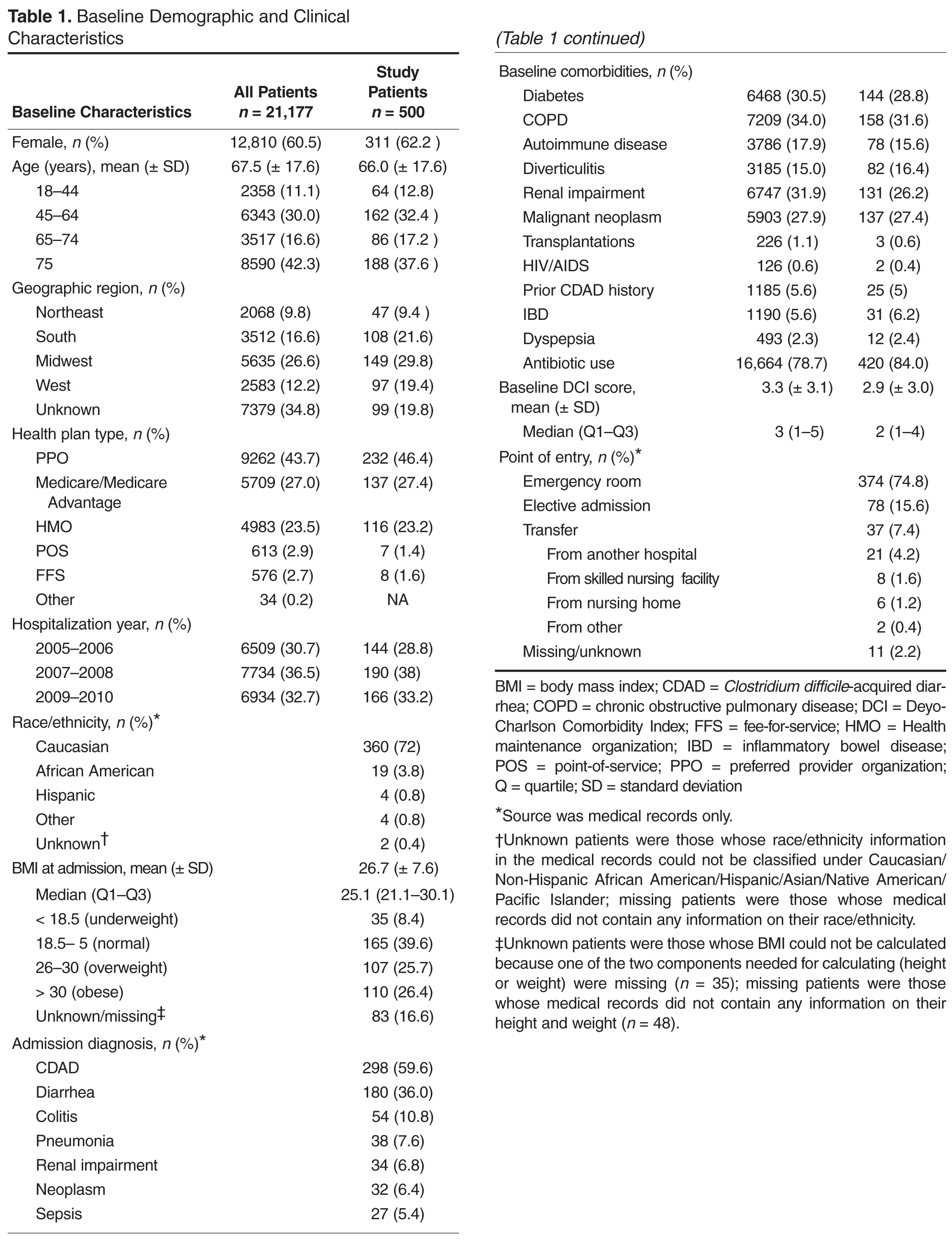
Consistent with the characteristics of the overall CDAD population within the original database, the randomly selected patients whose records were abstracted were predominantly women and elderly with a mean age of 66 (± 17.6) years (Table 1). Patients had a mean BMI of 26.7 (± 7.6), with 44% classified as being either overweight or obese. Most of the cohort had either CDAD or diarrhea as a primary diagnosis at admission. Among those with no admission diagnosis of CDAD or diarrhea, the mean time to CDAD acquisition was about approximately 1 week after admission.
CDAD Characteristics and Complications
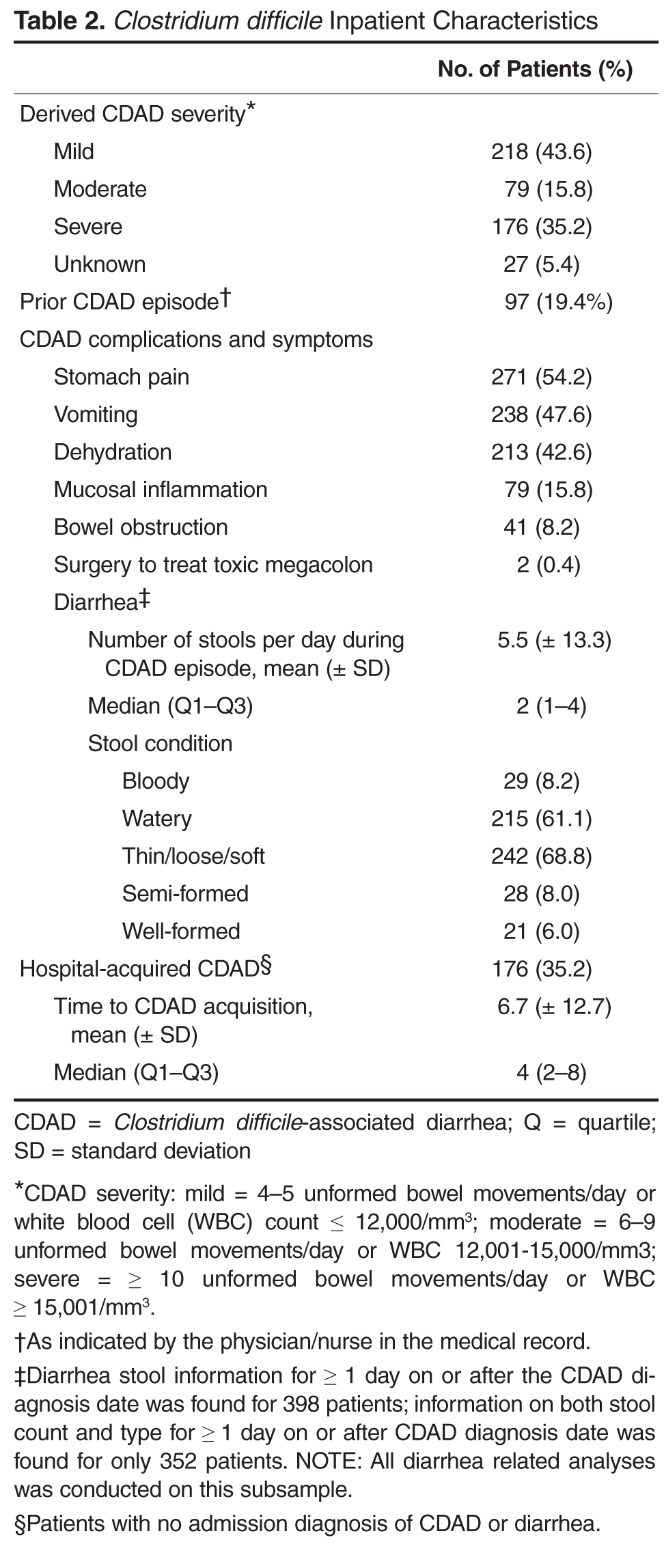
Using a derived definition of severity, most CDAD cases were classified either as
mild or severe (Table 2). For those with available diarrhea information, as expected the majority of patients reported thin/loose/soft or watery stools during the course of their CDAD episode. Patients had on average 5.5 (± 13.3) stools per day during the CDAD episode. In addition to diarrhea, stomach pain, vomiting, and dehydration were commonly reported. A relatively low proportion of patients had serious complications including mucosal inflammation and colectomy. One of every 5 patients was a recurrent CDAD case with documented prior CDAD.
CDAD-Related Resource Utilization
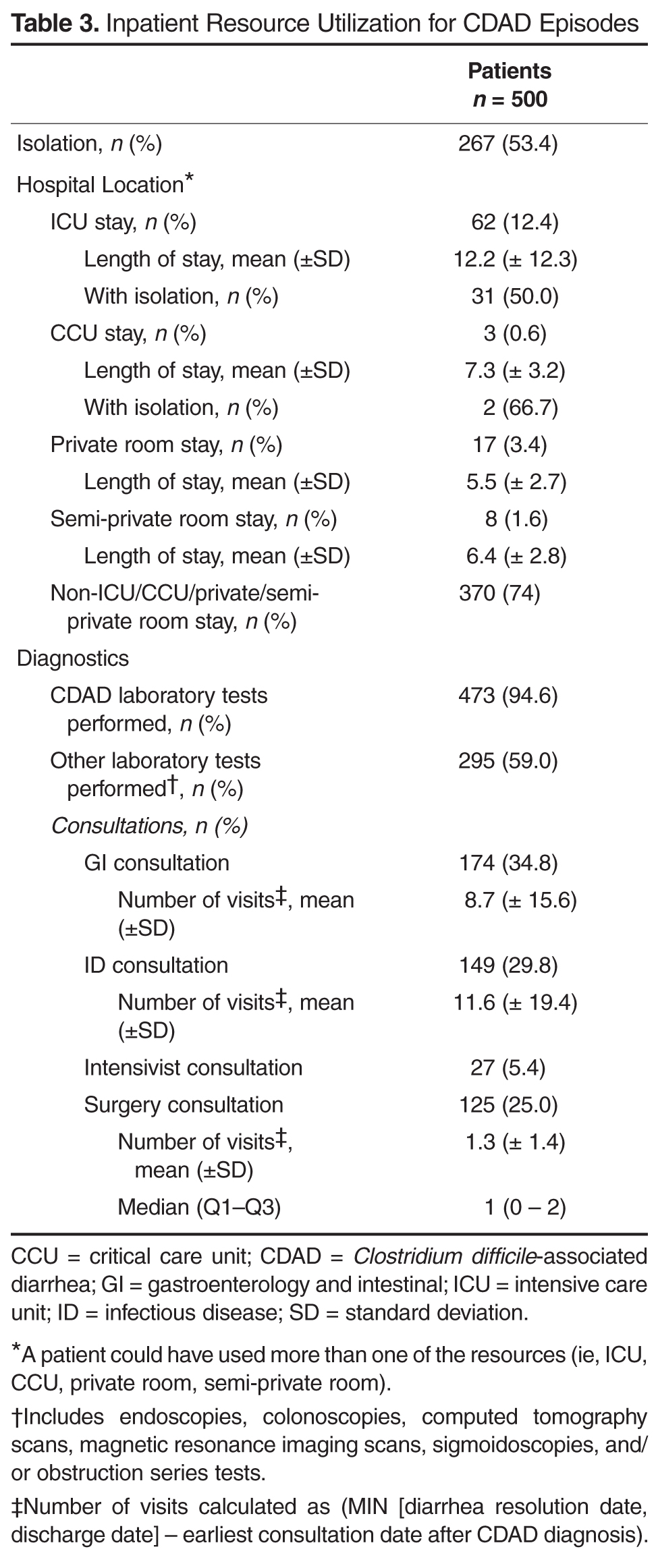
Following CDAD diagnosis, more than half of the study patients were isolated for 1 or more days. While the majority of patients with CDAD (74.0%) stayed in a general hospital room, 12.4% stayed in the ICU for a mean duration of 12.1 (± 12.3) days (Table 3). Half of these ICU patients required
isolation for at least 1 day. 5.6% stayed in the CCU in a private or semi-private room for 5 to 7 days during the CDAD episode.
About one-third of patients consulted a gastrointestinal or infectious disease specialist at least once. Among these patients, assuming that a patient following an initial specialist consultation would have follow-up visits at least once a day (formal or informal) for the remainder of the CDAD episode, we estimate that there were an average of 8.7 (± 15.6) and 11.6 (± 19.4) GI or ID specialist visits respectively during the CDAD episode.
Nearly all patients had their CDAD diagnosis confirmed by laboratory tests. CDAD virulence was identified as toxin A and/or toxin B in 47.6% of the samples. However, nearly three-fifths of patients also underwent 1 or more nondiagnostic tests including endoscopy, colonoscopy, computed axial tomography (CAT), or magnetic resonance imaging (MRI) scans, sigmoidoscopy, and/or other obstructive series tests during the CDAD episode.
CDAD Treatment
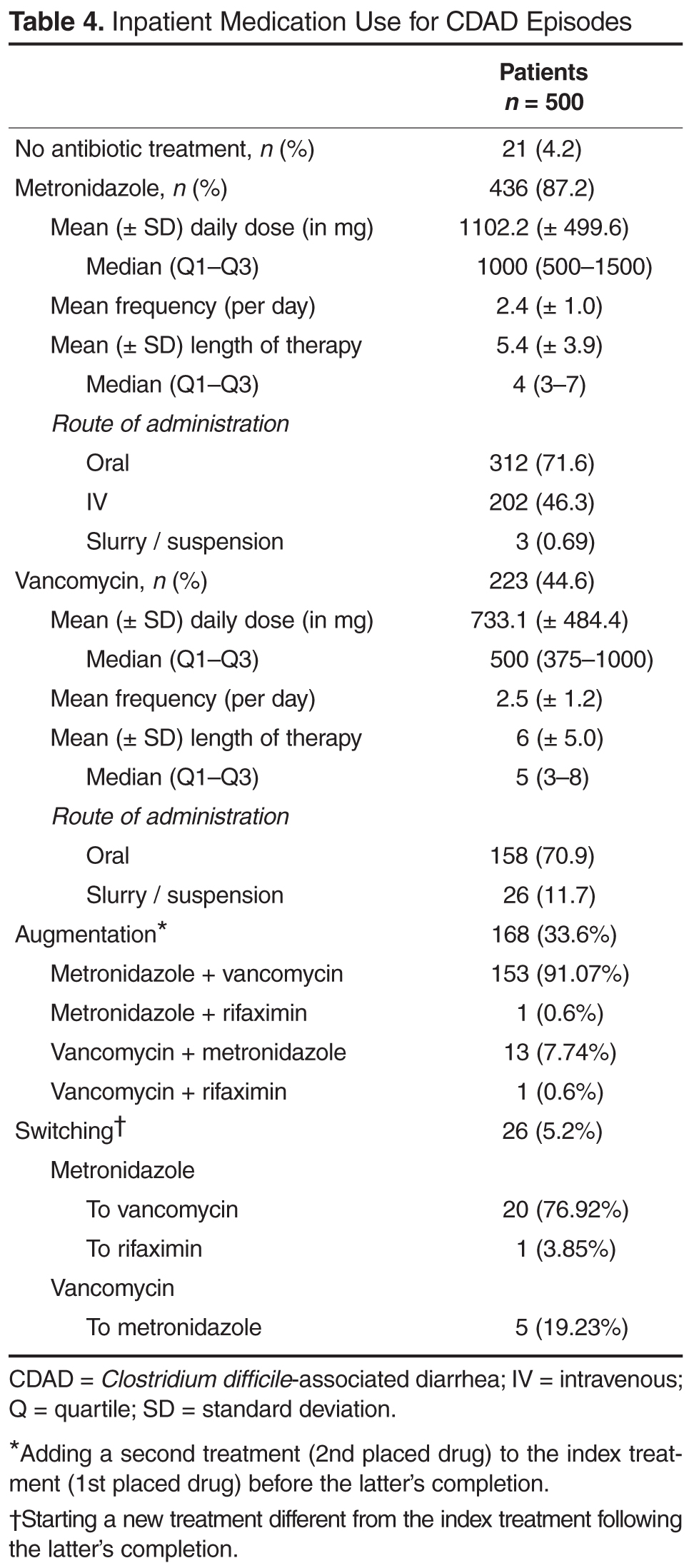
About 4.2% patients received no antibiotic treatment following CDAD diagnosis. Nevertheless, twice-daily metro-nidazole was the most frequently used antibiotic for CDAD (87.2%), with oral being the preferred route of administration among these patients. The median duration of treatment and daily dose were 4 (3–7) days and 1000 mg, respectively. Oral vancomycin was administered to nearly half of the patients for a median duration and daily dose of 5 (3–8) days and 500 mg, respectively; mean frequency of administration was 2.5 (± 1.2) times per day (Table 4). One-third of the patients (33.6%) augmented their first-line therapy, most frequently adding vancomycin to the initial metronidazole treatment or vice-versa. Only 5.2% of patients switched completely from the first-line therapy, predominantly from metronidazole to vancomycin (4%).
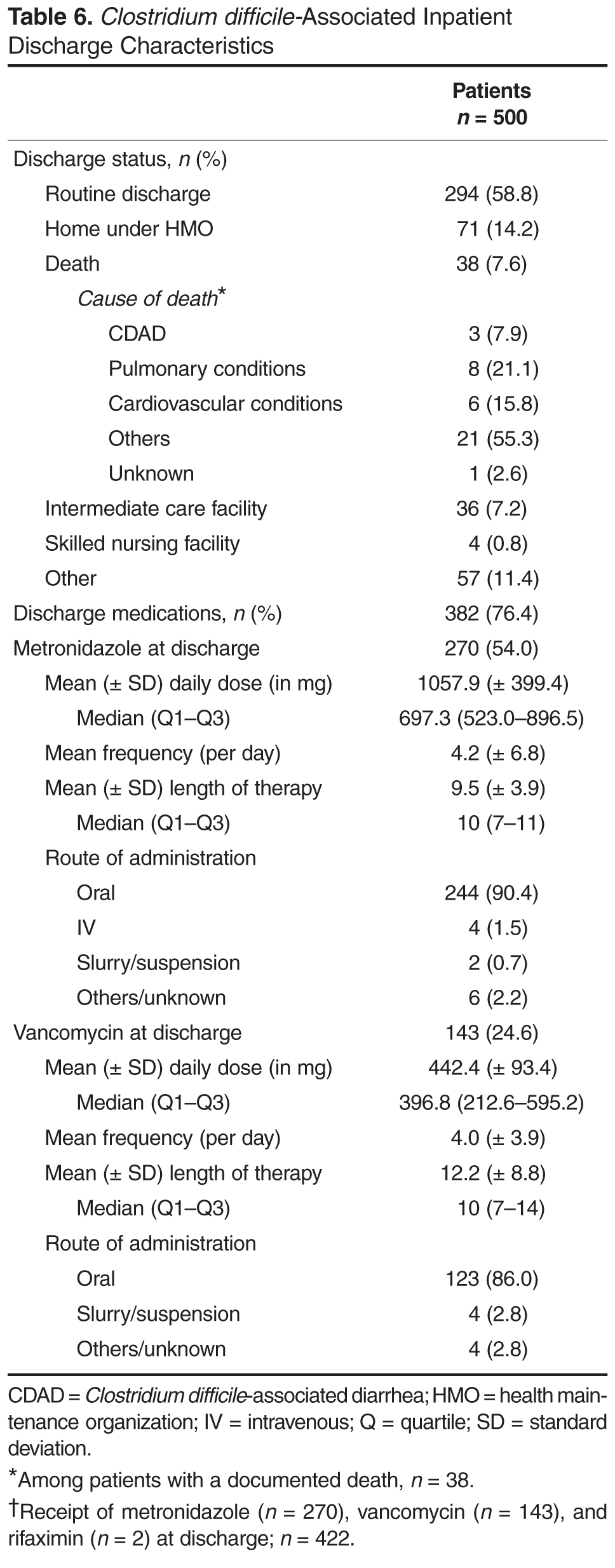
CDAD at Discharge
Overall, the mean time from CDAD diagnosis to hospital discharge was 8.8 (± 13.3) days (Table 5). Notably, CDAD was documented to persist in 84.4% of patients at the time of discharge, with 82.5% of patients obtaining prescriptions for post-discharge antibiotic treatment involving metronidazole, vancomycin, or rifaximin (Table 6). Among the 7.6% of patients who died while hospitalized, CDAD was identified as the cause of death in one-fifth of these cases.