Nonpharmacologic Treatment of Chronic Pain—A Critical Domains Approach





What strategy can be recommended to help patients regain function?
Regaining Function
Pain is disruptive. Patients with pain may avoid activity due to fear of re-injury or making the pain worse. Pain may keep them awake at night and lead to daytime fatigue. Pain can be so bad that a patient cannot even do simple tasks, One of the most important goals in successfully managing pain is to move away from trying to cure the pain and instead focus on regaining function—helping the patient do some of the things he/she really wants to do despite the pain. The patient may not be able to all the things he/she used to do, but new ways to do many of these activities can be found. Patients can also identify new rewarding activities to do now that things have changed.
To regain function, an evidence-based strategy comes from behavior therapy and is known as graded activation [42–46]. Here the patient is assigned one very small, manageable and incremental step towards achieving a goal. As these small goals are met, the patient feels motivated to engage in more and larger goals.
Lisa specifically mentioned giving up valued activities in light of her chronic pain. To help her re-engage a graded task assignment approach can be taken. For example, Lisa would be encouraged to first identify an activity she would like to get back to doing again. If she were to say “gardening,” then she is to next identify one small, specific, and easily achievable goal for the short term, such as “garden for 20 minutes at least once in the next week.” Help her identify the roadblocks to completing this small goal and brainstorm solutions such as “My kids have soccer and basketball practices 5 days next week so I will ask my ex-husband take them to practice at least one day next week so I can spend time in my garden.” Lisa will be told to schedule time to garden as if it were an appointment with a doctor.
Another important issue to consider is the tendency for inconsistent levels of activities across days that are predicated on how one feels that particular day. On “good days” often patients inadvertently engage in more activity than personal limitations allow and as a consequence experience several “bad days” of pain and other symptom flare up which can result in lost productivity and worse self-esteem. The goal is to have patients engage in a moderate amount of activity every day and avoid activity “binges” or days with little of no activity. Graded activation is a method of pacing that can improve physical functioning while minimizing the likelihood of pain flare-ups.
What simple strategies can be used to improve patients’ emotional well-being?
Emotional Well-Being
Psychological distress and emotional well-being occur along a continuum. Eliminating psychological distress only returns one to a state of being without distress. That is not the same as experiencing emotional well-being or happiness. People with chronic pain who also have higher levels of emotional well-being (or happiness) have decreased pain severity, fewer symptoms, better levels of functioning, and greater life satisfaction [47–49].
Recent studies provide preliminary evidence suggesting that resilience-based interventions such as keeping a gratitude journal or scheduling time to engage in pleasant activities boast equivalence or even superiority to CBT for the treatment of mood with effects that persist over time [50,51]. Two recent meta-analyses have shown that resilience-based interventions have been used to treat healthy individuals and a range of clinical conditions with a mean effect size for improving well-being ranging between 0.34 to 0.61 (ie, moderate-large effects [Cohen’s d]) [52,53]. Positive activities interventions are thought to function by increasing positive affect, which in turn, enables creativity, problem-solving, perspective-taking, and other beneficial states [54]. Such states are conducive to better mood [55,56], behavioral activation/increased physical activity [57–60], better sleep [61–63], increased social support [54,64] and physiological changes (eg, improved vagal tone, lower blood pressure, more adaptive immune responses) [57,65–69]. Recent studies have successfully adapted resilience-based interventions and shown them to be effective for individuals with pain [70–72]. Resilience-based interventions may be particularly helpful for chronic pain patients given that depression and sleep disturbances are frequent comorbidities [5,21–26,28,73,74].
Lisa stated, “I have zero joy in my life…” and later burst into tears. It is easy to surmise that her emotional well-being is quite poor. She also noted that she saves all of her energy for her job and has “nothing left in the tank” for her children or herself. This is a common picture for individuals with chronic pain. Valued life activities like spending quality time with loved ones, going to sporting events or doing a hobby are put aside in favor of obligatory (eg, activities of daily living) and committed (eg, work, school) activities. While this strategy might help one survive, it certainly is not conducive to thriving. To help Lisa improve her emotional well-being, there are good data supporting pleasant activity scheduling amongst other strategies. For pleasant activity scheduling Lisa would be directed to set aside time a few days a week (at least an hour) to do things that she enjoys. This time should be placed on her calendar and treated with the same level of commitment as going to work or to an appointment with her physician.
What nonpharmacologic options are available to help improve patients’ sleep?
Sleep
Lisa indicated that she has trouble falling asleep and then when she does sleep, she usually wakes up feeling unrefreshed and irritable. This is a common complaint amongst individuals with chronic pain who often report difficulty falling asleep, being awakened by pain or discomfort and awakening feeling unrefreshed and unrestored [75]. Sleep, pain and mood form a symptomatic triad such that when one aspect is affected the others are impacted. For example, when Lisa does not sleep well, her pain and mood worsen, as well. Conversely, when her pain is better, she likely sleeps better and wakes up feeling less irritable and experiences less pain.
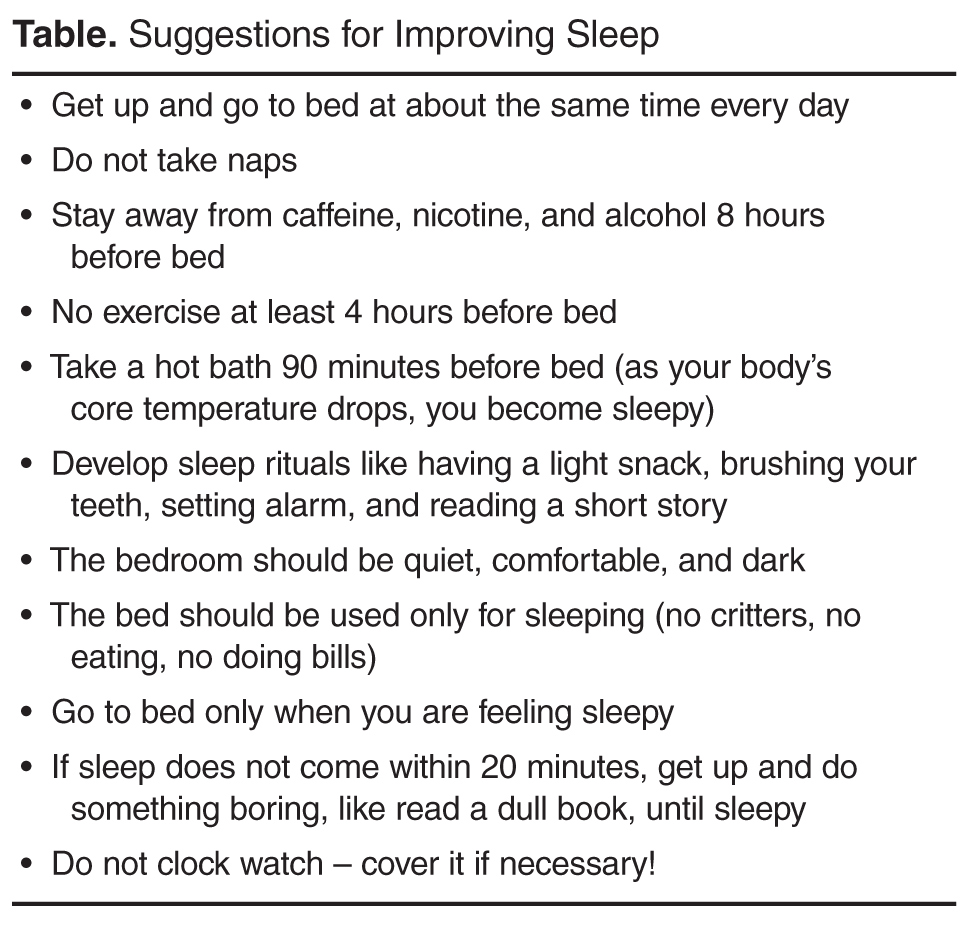
Behavioral strategies for improving sleep, if used on a regular basis, can help individuals get needed restorative sleep with the additional benefits of improving mood, pain, fatigue, and mental clarity [76]. Some of these behavioral strategies focus on maintaining regular sleep routines (go to bed at the same time every night even on weekends), engaging in sleep conducive behaviors (eg, attempting to sleep only when in feeling sleepy), and avoiding stimulating activities (eg, watching action movies, or consuming nicotine or caffeine). Studies have shown that behavioral strategies targeting sleep appear to have a direct impact on pain symptoms and on functional interference resulting from nonrestorative sleep [77,78].
What stress reduction strategies can be recommended to the patient?
Stress
Stress management has long been a target of treatment in patients with chronic pain. Progressive muscle relaxation (PRM) [79] and autogenic training have typically served as an important foundation of behavioral intervention for chronic pain [80] although there are no randomized controlled trials for PRM as a stand-alone intervention and two separate trials of autogenic training failed to find superiority for this intervention [81,82]. Despite the lack of direct evidence, clinical experience and the knowledge that both relaxation techniques are commonly part of CBT for chronic pain, their efficacy is generally accepted.
An emerging area of nonpharmacologic treatment is mindfulness-based interventions [83], which can include mindfulness-based stress reduction (MBSR) and Acceptance and Commitment Therapy [84], which can be considered a hybrid between mindfulness meditation and CBT. These interventions are still relatively new and larger, better controlled studies are needed. In MBSR, the patient is directed to focus on one thing such as a sound, a pleasant scene or their own breathing. The practitioner is encouraged to keep thoughts present oriented and analytical concerns are to be gently dismissed in favor of focusing on the sounds, scene, or breath. A recent meta-analysis evaluating 15 studies in clinical populations reported that there were small to medium effect sizes for patients with chronic pain [85]. In another new meta-analysis evaluating only studies in chronic pain the authors reported that sleep quality and pain acceptance were the 2 variables with the largest effect sizes based on the 11 studies they evaluated [83]. Similarly, a meta-analysis that included both MBSR and ACT found that 22 studies of varying quality suggest significant but small effect sizes for pain (ES = 0.37) and depression (ES = 0.32) [86]. They concluded the mindfulness-based treatments were not superior to CBT but could be a viable alternative.
For Lisa and many other chronic pain patients, the symptom flares seem to coincide with periods of stress. These flare ups are not inconsequential and have cost her days of lost productivity and potentially put her employment at risk. Moreover, she has identified stress as a trigger for over-eating which certainly contributes to her weight problems and low self-esteem. MBSR can be learned in a structured class or online--many of the principles can be taught by lay instructors.
Summary
While it is likely that health care professionals will continue to rely on pharmacological therapies in treating chronic pain, it is important to be aware that reliance on medications and procedural interventions alone is unlikely to bring adequate relief to individuals living with chronic pain [1]. Optimal pain management appears to be achieved by using a combination of both pharmacologic and nonpharmacologic approaches. Nonpharmacologic interventions that actively engage the patient in pain management such as exercise, behavioral activation, sleep hygiene and stress management are relatively easy to implement and do not necessarily require the expertise of mental health professionals. The challenge is considering pain in its biopsychosocial contexts and defining an approach that is both comprehensive and feasible. Using the ExPRESS domains to help guide care can provide a road map.
Corresponding author: Afton L. Hassett, PsyD, 24 Frank Lloyd Wright Drive, Lobby M, CPFRC, Ann Arbor, MI 48106, afton@med.umich.edu.