Postpartum Recovery Trends in Women with Hypertensive Disorders of Pregnancy





Main Outcome Measure
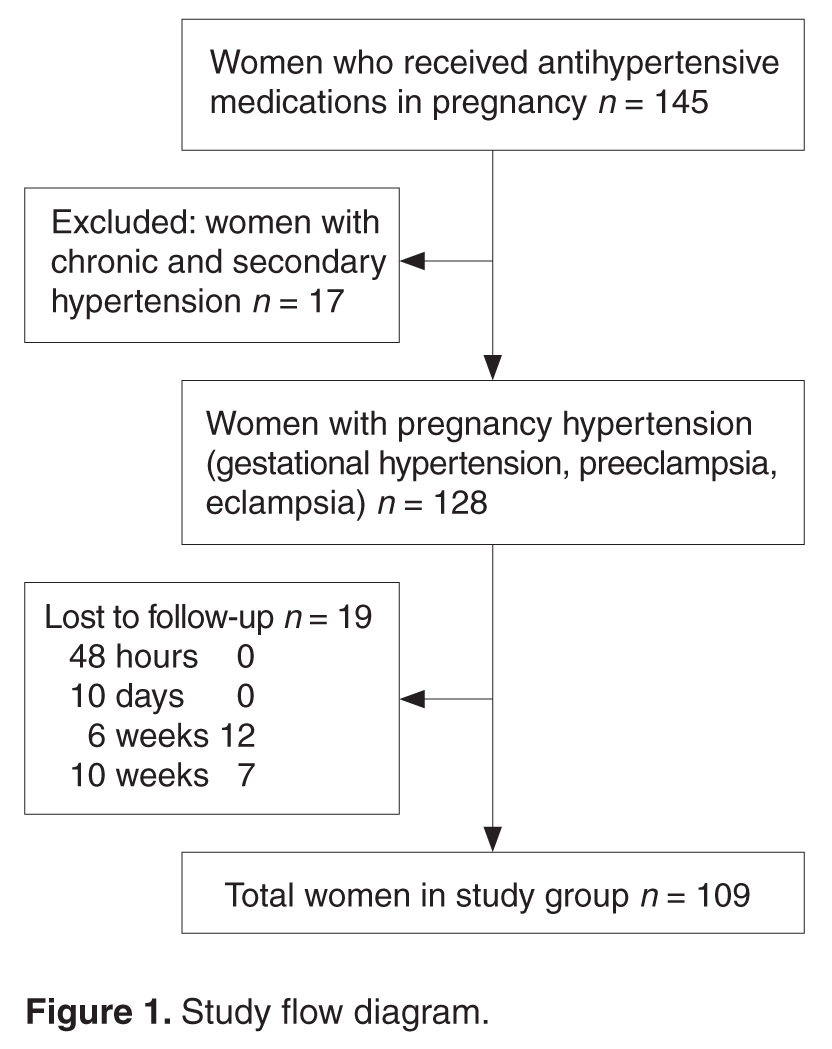
Time to reversion of hypertension was the main outcome measure. We defined the reversion date as the day that hypertension medications were stopped. This information was obtained via in-person questioning on the 2nd postpartum day and at the 6-week postnatal visit and via telephonic survey on the 10th postnatal day and at 10 weeks postdelivery. Women who missed the 6-week postnatal visit were also followed up by telephone.
Data Collection
Demographic details (age, parity, BMI) as well as information regarding gestational age at onset of hypertension, severity, highest systolic and diastolic blood pressure recordings, treatment received, complications related to hypertension, pregnancy termination and delivery was obtained from the medical charts and/or via telephonic follow-up.
Analysis
We used Pearson’s chi-square test to assess the association between recovery trends in blood pressure and the patient’s demographic profile and details of pregnancy hypertension. Statistical analysis was done using SPSS16.
Results
In our study, earlier the gestational age at onset of hypertension and earlier gestation at delivery was associated with slower recovery from hypertension (Table 2). Time taken for recovery also was associated with age, BMI, severity of hypertension, associated complications, and the number of antihypertensive medications received (Table 2). Among women who received more than 3 antiphypertensives in pregnancy, nearly 50% continued to have hypertension beyond 6 weeks (Table 2). 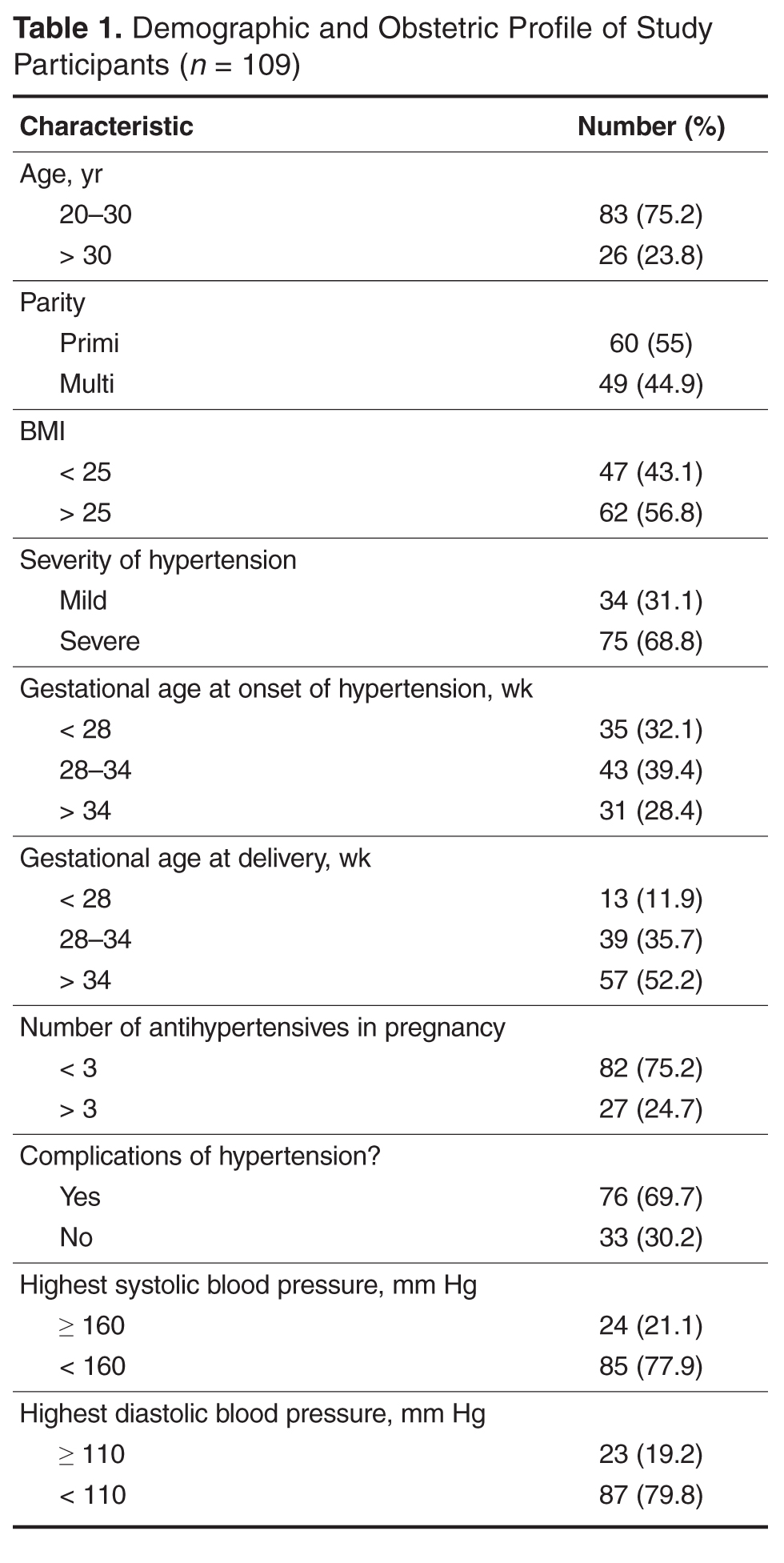
On testing for strength of correlation, it was found that body mass index and time to blood pressure normalization had a strong positive correlation (r = 0.8). The remaining parameters (ie, gestational age at onset, gestational age at delivery, severity and complications of hypertension and number of antihypertensive medications) and time to recovery were weakly correlated (r = 0.3 to 0.5 [+/–]).
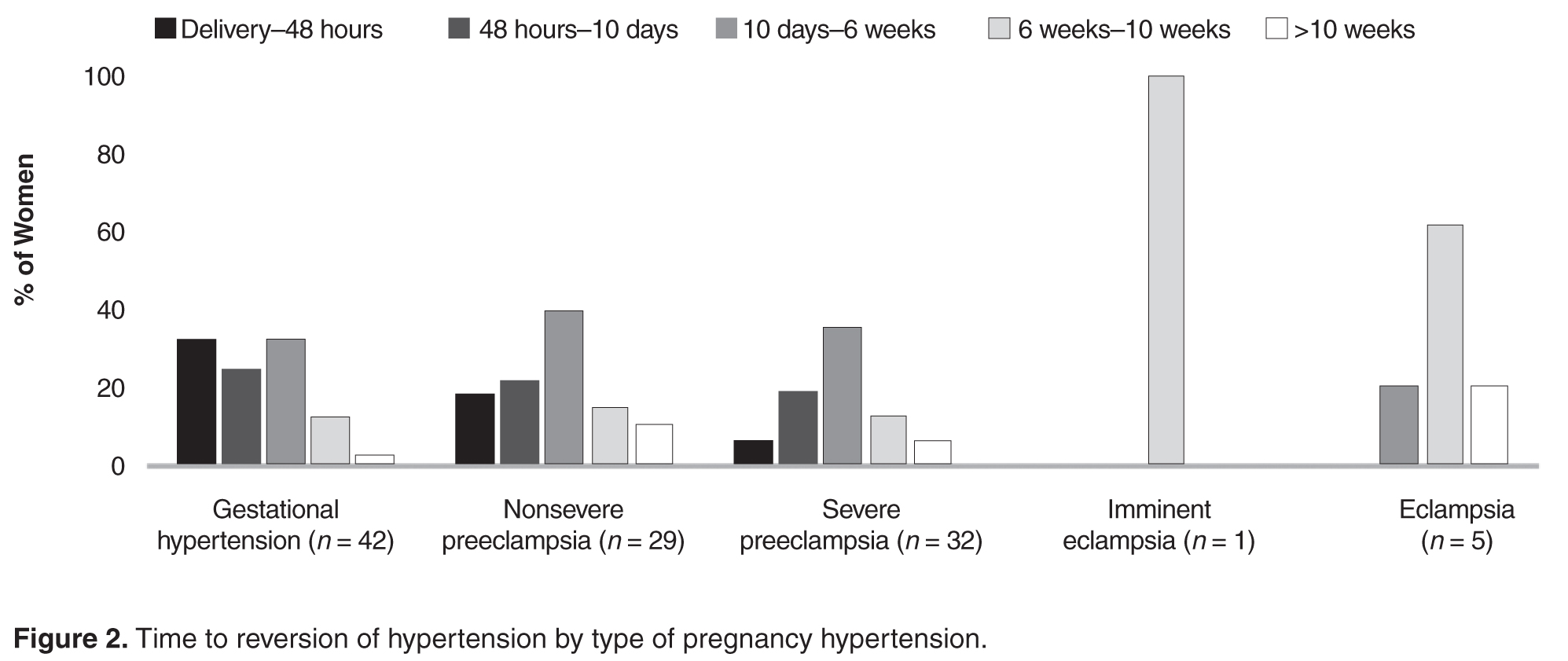
Women with gestational hypertension and mild preeclampsia had faster normalization of blood pressure compared to those with severe preeclampsia and eclampsia (Figure 2). Only 15% of women with gestational hypertension had persistent hypertension beyond 6 weeks, whereas in the groups with nonsevere preeclampsia, severe preeclampsia, and eclampsia, blood pressure 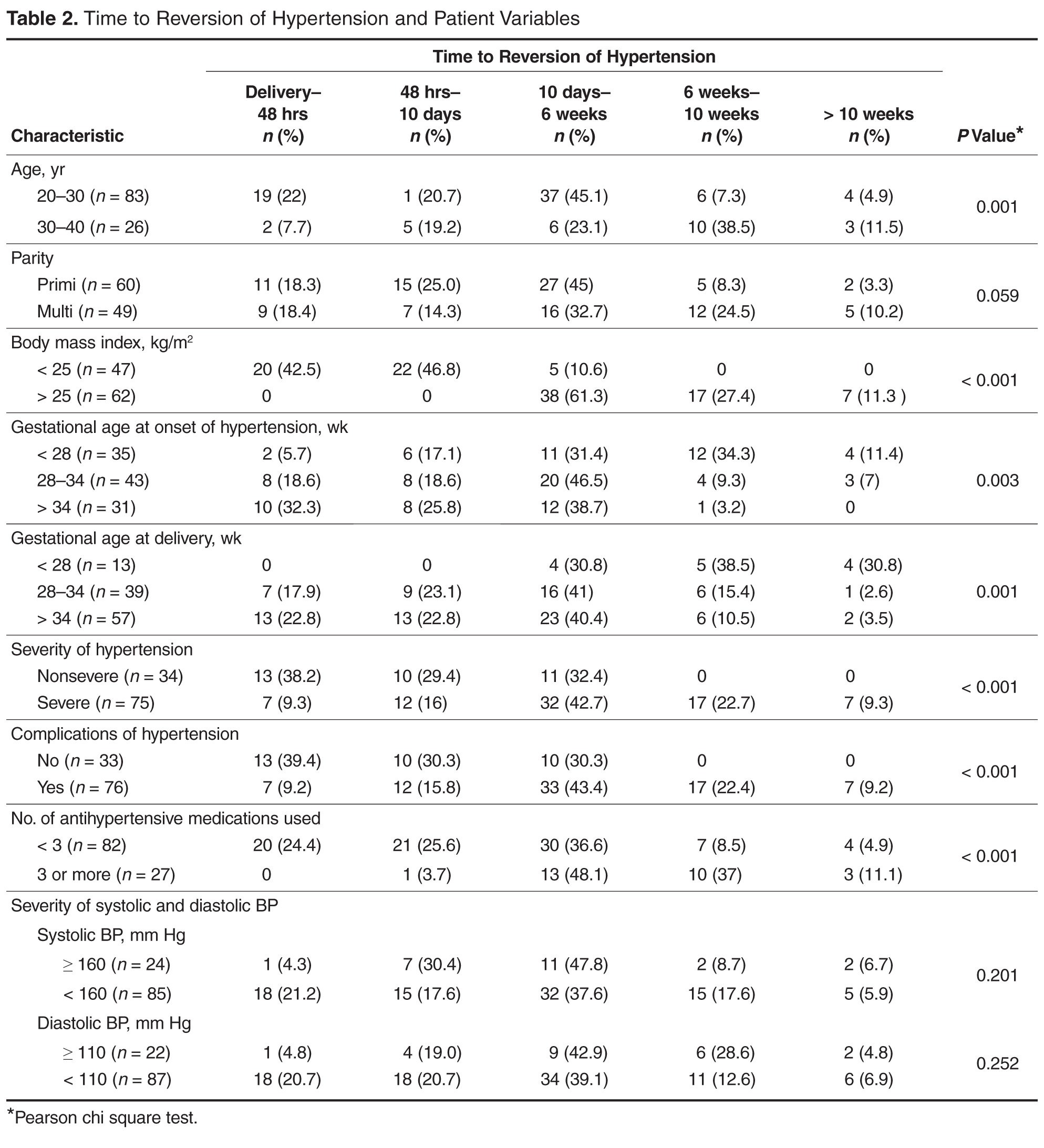
Eighteen women had additional medical problems: gestational diabetes (n = 5), anemia (n = 3), hypothyroidism (n = 4), rheumatic heart disease (n = 2), antiphospholipid antibody syndrome (n = 1) chronic kidney disease (n = 1), post atrial septal defect closure (n = 1), and tricuspid valve prolapse (TVP) with regurgitation and pulmonary arterial hypertension (n = 1). With the exception of the woman with chronic kidney disease, all reverted to normal blood pressure by 6 weeks; the woman with TVP reverted after corrective cardiac surgery in puerperium.

Discussion
In the present study we assessed possible correlations of obstetric profile with time to postpartum recovery of blood pressure in women with pregnancy hypertension. Women with advanced age, higher body mass index, early gestational age at the onset of hypertension, early gestational age at delivery, severe hypertension, and those with complications of hypertension took longer time in the postnatal period for normalization of blood pressure.