Supporting the Needs of Stroke Caregivers Across the Care Continuum





Positive effects of caregiving have also been reported, including a feeling of confidence, satisfaction in providing good quality care [30,39,40], an improved relationship with the care recipient [30,40,41], having greater life appreciation, and feeling needed and appreciated [40]. In a systematic review of 9 studies, improvements in the stroke survivor’s condition was a source of positive caregiving experiences [40]. In 2 studies, two-thirds of caregivers surveyed affirmed all survey items related to positive aspects of caregiving [30,42]. Additionally, studies have demonstrated that caregivers who engaged in emotion- and problem-focused coping strategies had positive caregiving experiences [40]. Haley et al found that by 3 years post-stroke many of the ill effects of caregiving had resolved, suggesting that some caregivers may be successful in adapting to their “new” post-stroke lives [23].
Understanding the difficulties and issues faced by caregivers throughout the trajectory, from immediately following the stroke through the transition home and, ideally, the adaptation of the caregiver to this new life, provides an opportunity for health care professionals to intervene with strategies to support this major life change.
Caregiving Trajectory and Ongoing Needs of Stroke Caregivers
Stroke survivors and their family caregivers rapidly move from intensive therapy and nursing case management while in a facility to little or no assistance following discharge. Despite case management and discharge planning services received while in an institutional setting, the transition from inpatient care to home can be a crisis point for caregivers [9]. They describe having to figure things out for themselves with little or no formal support after discharge [9,43,44], leaving them feeling overwhelmed, exhausted, and abandoned once they return home [9].
These family members rarely make an active choice to become caregivers; rather, they take on the role because they are unable to perceive or access any other suitable alternatives [8,45]. Whatever their circumstances, these devoted family members are particularly vulnerable as they transition into the caregiving role without an adequate support system for assessing and addressing their needs [7–9,46]. Without this assistance, caregivers develop their own solutions and strategies to meet the needs of the care recipient after discharge [47,48]. Unfortunately, these strategies are often ineffective and may result in safety risks for patients (eg, falls, skin breakdown, choking), and care-related injuries (eg, falls, muscle strains, bruises) and increased stress and anxiety for caregivers [48–50].
Caregivers have described unmet needs in many domains including skills training, communicating with providers, resource identification and activation, finances, respite, and emotional support [35,44,48,51,52]. Bakas et al found that in the first 6 months post-discharge, stroke caregivers had needs and concerns related to information, emotions and behaviors, physical care, instrumental care, and personal responses to caregiving [48], and that their information needs change during the course of the patient’s recovery [53]. In a study by Lutz et al [44], caregivers identified multiple areas where they felt they were unprepared to assume the caregiving role post-discharge. These included identifying and activating resources; making home and transportation modifications to improve accessibility; developing skills in providing physical care and therapies; managing medications and behavioral issues; preventing falls; coordinating care across settings; attending to other family responsibilities; and caring for themselves.
In a study of interactions between rehabilitation providers and stroke caregivers, Creasy et al [52] noted that caregivers have needs, which were often not recognized, in the following areas: information; providing emotional support for the stroke survivor and having their own emotional support needs met; being involved in treatment decisions; and being adequately prepared for discharge home. Caregivers’ interaction styles with providers, which ranged from passive to active/directing, affected their abilities to have their needs recognized and addressed. These findings highlight the importance of recognizing the caregiver’s interaction style and tailoring communication strategies accordingly.
Cameron et al [54] noted that caregiver support needs change over time, with needs being highest during the inpatient phase as they prepare for discharge home. Moreover, caregivers who are providing care for stroke survivors with more severe functional limitations need more support over a longer period of time. Recognizing the needs of stroke caregivers, the 2016 Canadian Stroke Best Practice Recommendations on Managing Transitions of Care Following Stroke includes recommendations related to assessing, educating, and supporting stroke family caregivers [55].
Assessing Caregiver Readiness and Related Outcomes
Young et al [58] recommend specific domains for a comprehensive readiness assessment of stroke family caregivers. Caregiver domains include strength of the caregiver/care recipient relationship; caregiver willingness to provide care; pre-existing health conditions, previous responsibilities, caregiving experience, home and transportation accessibility, available resources, emotional response to the stroke, and ability to sustain the caregiving role. This type of readiness assessment should be completed early in the care trajectory, while the stroke survivor is receiving inpatient care, so that care plans can be tailored to address gaps in caregiver preparation prior to discharge. It is especially important for new caregivers and those caring for stroke survivors with significant functional limitations [44]. Currently there are no tools designed to assess a family member’s readiness to assume the caregiver role.
Validated instruments have been developed to assess caregiving outcomes, including preparedness, with caregivers who have been providing care for a period of time. For example, the Mutuality and Preparedness Scales of the Family Caregiver Inventory was developed with caregivers 6 months post-discharge [59] and has been validated with stroke caregivers at 3 months post-discharge [60].
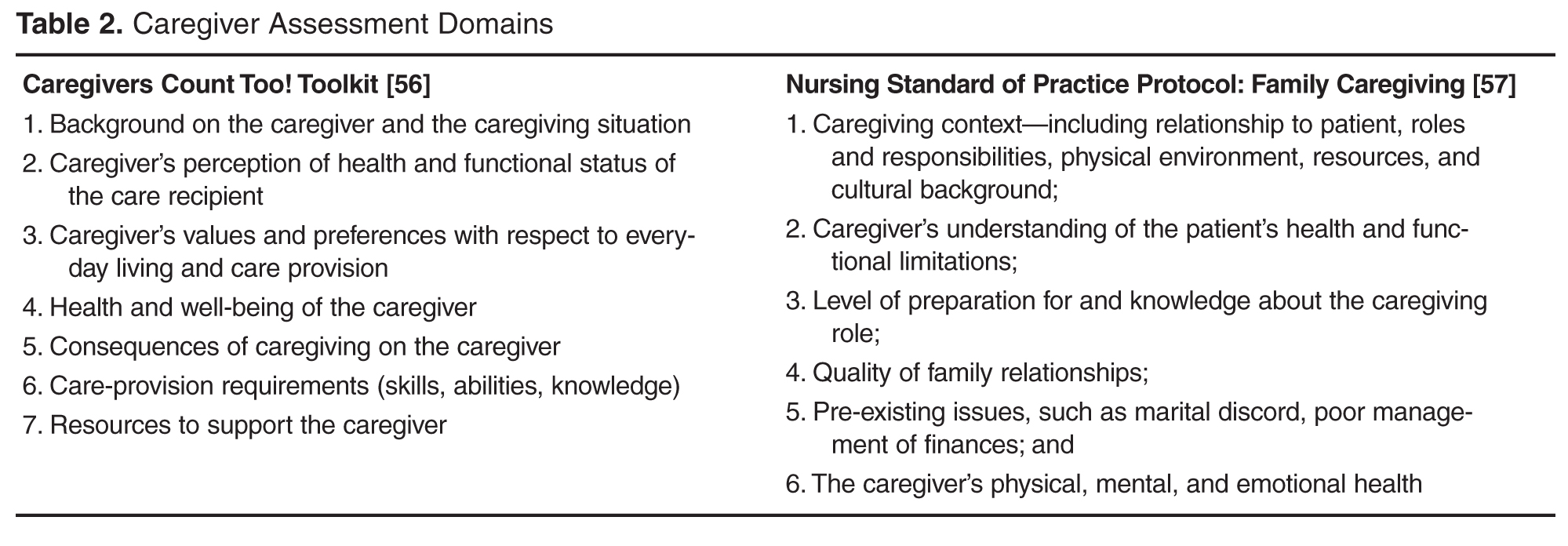
Several validated tools are available to assess the caregiver’s changing needs and the effects of care provision on well-being [8,45,61]. For example, the Caregiver Strain Index [62] has been validated in studies with stroke family caregivers [11,28]. Bakas developed 2 scales to specifically assess stroke caregivers post-discharge. The Bakas Caregiving Outcomes Scale assesses caregiver life changes [63] and the Needs and Concerns Checklist assesses post-discharge caregiver needs [48]. There are many other instruments designed to assess general caregiving outcomes, including depressive symptoms, burden, anxiety, and well-being. For a list relevant tools see Deeken et al [61] and The Selected Caregiver Assessment Measures from the Family Caregiver Alliance [64].
While these scales are helpful for assessing caregivers who are already providing care, they do not capture the gaps in caregiver readiness prior to patient discharge from the institutional setting. Taken together, these studies suggest that assessing readiness and implementing interventions to improve caregiver preparation prior to discharge and assessing and addressing their changing needs over time, from inpatient care to community reintegration, may be important strategies for improving both caregiver and stroke survivor outcomes. These strategies may also facilitate sustainability of the caregiver role over time.