Measurement of physical activity and sedentary behavior in breast cancer survivors






Background Breast cancer survivors’ self-perceived physical activity (PA) and sitting time (ST) may differ significantly from the general population and other survivor groups, so it is important that PA and ST measurement tools are compared within the breast cancer survivor population.
Objective To compare accelerometer and self-report estimates of PA and ST in breast cancer survivors.
Methods 414 breast cancer survivors (age, 56.8 years [SD, 9.2 years]; BMI, 26.2 kg/m2 [5.4 kg/m2]) wore an accelerometer for 7 consecutive days and completed a modified Godin Leisure-Time Exercise Questionnaire (GLTEQ), the International Physical Activity Questionnaire (IPAQ), and the Sitting Time Questionnaire (STQ) which all measured hours/minutes of activity/sitting per day. Mean differences and correlations of ST, light PA (LPA; ≤1.5 metabolic equivalents [METs]), and moderate and vigorous PA (MVPA; ≥3 METs) were compared using random-intercept mixed-effects regression models and the Spearman rank correlation coefficient (Spearman’s rho [rs], where rs = 1 means a perfect positive correlation, and rs = -1 means a perfect negative correlation).
Results Mean daily durations of MVPA were: accelerometer, 20.2 minutes; GLTEQ, 23.6 minutes (Pdiff = .02); and IPAQ, 87.4 minutes (Pdiff < .001). Correlations between accelerometer-estimated MVPA were moderate for the GLTEQ (rs = 0.56) and poor for the IPAQ (rs = 0.02). Mean daily durations of LPA were 239.5 minutes for the accelerometer and 15.4 minutes for the GLTEQ (Pdiff < .001); the measures were not correlated (rs = 0.004). Mean daily durations of ST were: accelerometer, 603.9 minutes; STQ, 611.8 minutes (Pdiff = 0.9); and IPAQ, 303.8 minutes (Pdiff < 0.001). Correlations with the accelerometer were fair (STQ: rs = 0.26; IPAQ: rs = 0.30). Differences in estimates varied by disease stage, age, presence of chronic conditions, and race.
Limitations Participants were predominantly white, highly educated, and high earners, which reduced generalizability.
Conclusions Congruency of measurement was dependent on tool, intensity of activity, and participant characteristics. Target outcome, implementation context, and population should be considered when choosing a measurement for physical activity or sitting time in breast cancer survivors.
Funding National Institute on Aging: #F31AG034025 (Dr Phillips), #AG020118 (Dr McAuley); National Cancer Institute: #K07CA196840 (Dr Phillips), #T32CA193193 (Dr Welch).†
Accepted for publication December 2, 2017
Correspondence whitney.welch@northwestern.edu
Disclosures The authors report no disclosures/conflicts of interest.
Citation JCSO 2018;16(1):e21-e29
†See Acknowledgment at end of article.
©2018 Frontline Medical Communications
doi https://doi.org/10.12788/jcso.0387
Related article
Effects of exercise interventions during different treatments in breast cancer
Submit a paper here
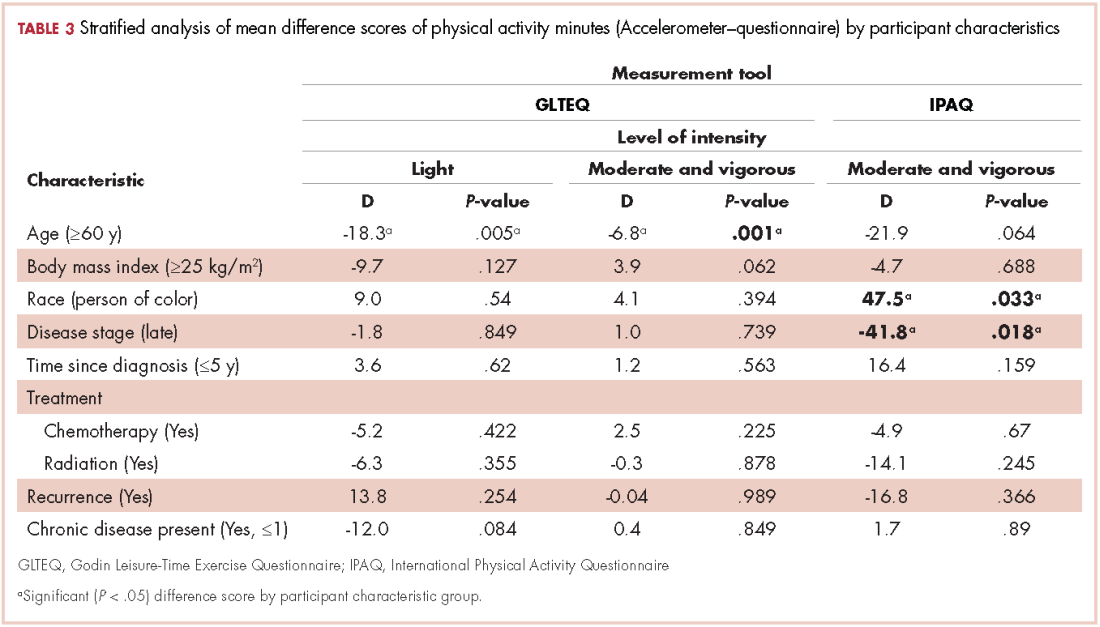
We calculated the measurement tool difference scores for each estimated intensity category (ST, LPA, MVPA), that is, accelerometer estimated ST minus STQ estimated ST, and GLTEQ estimated MVPA minus IPAQ estimated MVPA. We used these data in an exploratory analysis to examine whether there were statistically significant differences between measurement difference scores by demographic or disease characteristics using linear regression stratified analyses. For example, we were interested in whether there was a significant difference in measurement tool estimates for sitting time in older compared with younger survivors. Analyses were stratified by age (<60/≥60 years), body mass index (<25 kg/m2/≥25 kg/m2), race (white/people of color), disease stage (I and II/III and IV), years since diagnosis (≤5 years/>5 years), recurrence (Yes/No), received chemotherapy (Yes/No ), received radiation (Yes/No ), and the presence of 1 or more chronic diseases (Yes/No ).
Results
Participants
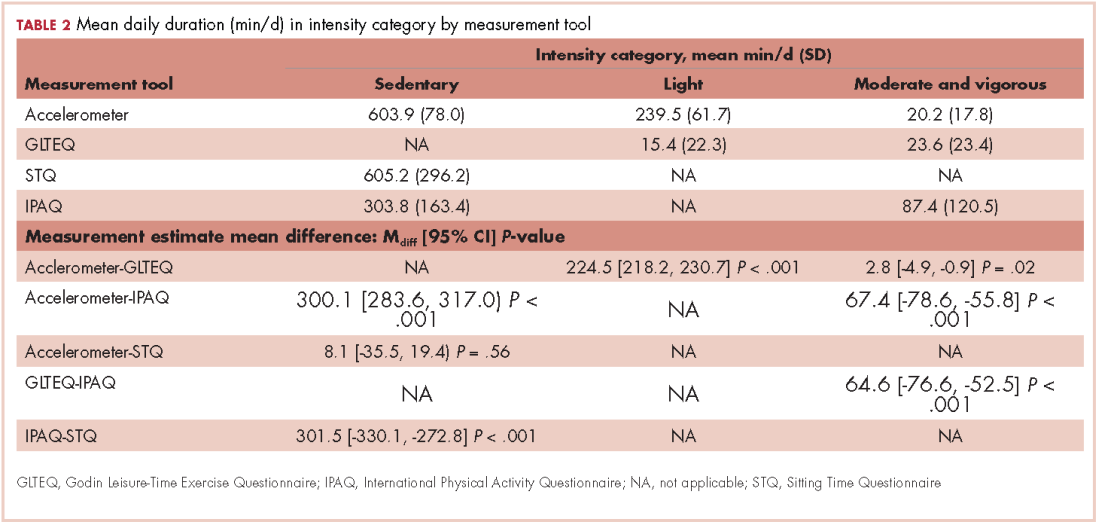
The mean age of the participants was 56.8 years [9.2], they were overweight (BMI, 26.2 kg/m2 [5.4]), and predominantly white (96.7%; Table 1). Table 2 provides a summary of mean daily duration of activity estimates for ST, LPA, and MVPA and the estimate mean difference scores between measurements.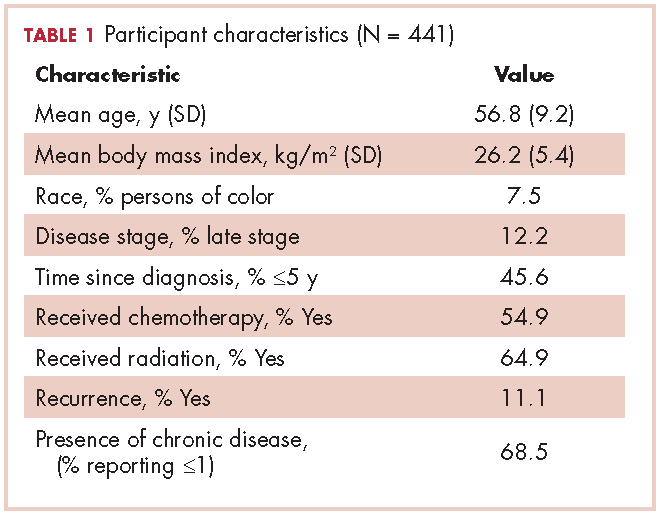
Moderate and vigorous physical activity
Accelerometer−GLTEQ. The mean difference in MVPA estimates between the accelerometer and GLTEQ was less than 5 minutes (Maccelerometer = 20.2 minutes; MGLTEQ = 23.6 minutes), even though the difference was statistically significant (P = .02). Estimates of MVPA from the accelerometer and GLTEQ (rs = 0.564, P < .001) showed a strong relationship. Stratified analyses showed that the difference scores between the GLTEQ and accelerometer were lower for older survivors (≥60 years) compared with younger survivors such that older survivors reported significantly less time in MVPA on the GLTEQ compared with accelerometer estimates (difference score [D] = 6.8 minutes less, P = .001).
Accelerometer−IPAQ. The accelerometer estimated significantly fewer minutes of MVPA per day when compared with the IPAQ (Mdiff = -67.4; 95% confidence interval [CI], -78.6, -55.8; P < .001). Estimates of MVPA from the accelerometer and IPAQ (rs = 0.011, P = .680) were poorly related. Differences between the IPAQ and accelerometer were greater for later-stage breast cancer, compared with early-stage diagnoses such that participants with late-stage disease reported significantly less MVPA on the IPAQ compared with accelerometer estimates (D = 41.8 minutes less than early-stage disease, P = .018). Finally, participants of color reported a greater difference in MVPA between the accelerometer and the IPAQ than did their white counterparts (D = 47.5 minutes, P = .033).
GLTEQ−IPAQ. GLTEQ estimated significantly fewer minutes of MVPA per day compared with the IPAQ (Mdiff = -64.6; 95% CI, -76.6, -52.5; P < .001). The estimates of MVPA from the GLTEQ had a small correlation with IPAQ estimates (rs = 0.128, P = .011).
IPAQ estimates showed almost triple the MVPA minutes per day as were estimated by the accelerometer and GLTEQ. As the MVPA estimate for the IPAQ include nonleisure activities, we conducted a post hoc analyses that only included the leisure-time items from the IPAQ. Leisure-time only IPAQ items, estimates indicated survivors spent a mean 18.5 [SD, 14.2] min/day in MVPA. Although the magnitude of the difference between the accelerometer and GLTEQ estimates (~10 minutes) was much smaller using the leisure-time only IPAQ items, a repeated measures analysis of variance revealed there was still a significant difference between these estimates (P < .05 for both) and negligible correlation.
Light intensity physical activity
Accelerometer−GLTEQ. There was a large and significant difference between LPA estimates from the GLTEQ and accelerometer (Mdiff = 224.5; 95% CI, 218.2, 230.7; P < .001) with estimates from the accelerometer being higher than those for the GLTEQ. Additionally, the measurements showed a negligible correlation (rs = 0.004, P = .94). Difference scores for GLTEQ and accelerometer estimated LPA were significantly different by age, with survivors aged 60 years or older demonstrating a difference that was 18.3 minutes shorter (P = .005) than the difference in younger survivors (<60 years).
Sitting time
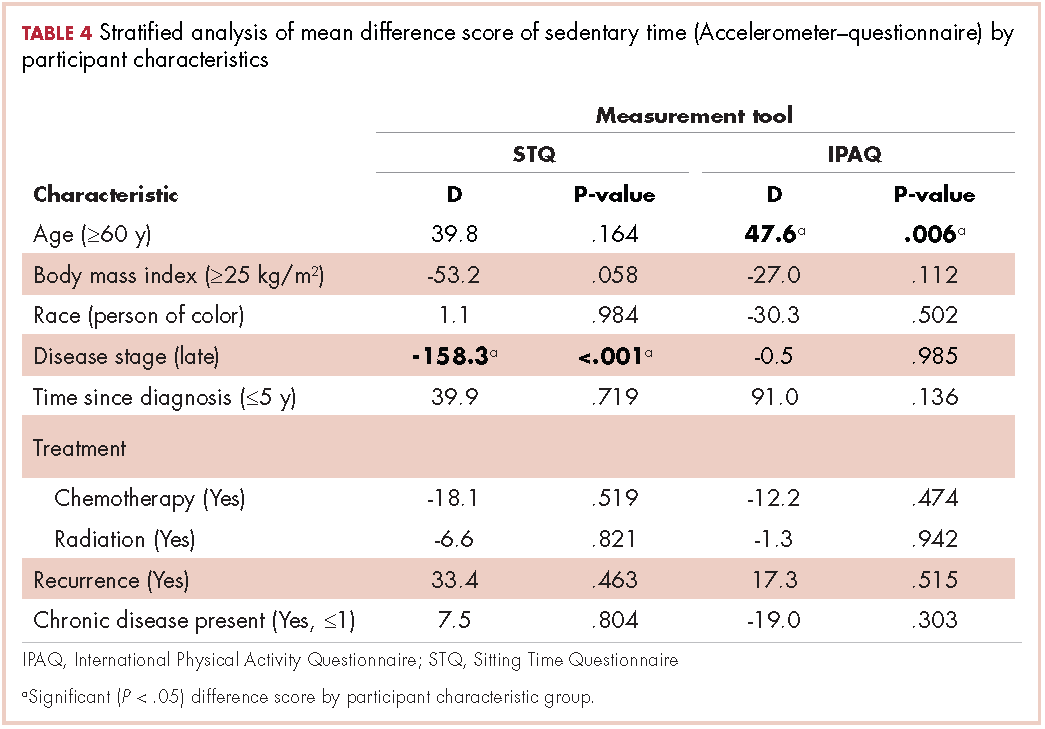
Accelerometer−IPAQ. Mean IPAQ estimates were significantly lower (M = 303.8 [63.4]) than accelerometer estimates (M = 603.9 [78.0]). Rank-order correlations between IPAQ and accelerometer estimated ST was small (rs =0.26, P < .001). Difference scores between IPAQ and accelerometer estimates were significantly greater for survivors who were 60 years or older, compared with those younger than 60 years (D = 47.6 minutes, P = .006), indicating that older survivors tended to self-report significantly more ST than estimated by the accelerometer.
Accelerometer−STQ. There was no significant difference in estimated mean ST minutes per day between the STQ and the accelerometer, but the correlation between estimates was low (rs = 0.30, P < .001). Stratified analyses revealed estimates for the difference scores for mean daily ST between the STQ and accelerometer were greater for participants who were diagnosed with later-stage breast cancer (D= -158.3 minutes, P < .001) and those who had received chemotherapy (D= -61.7 minutes, P = .028; Table 2) than for those who were diagnosed with early-stage breast cancer or had not received chemotherapy. Women who had later-stage disease reported significantly less ST than did women diagnosed with early-stage disease, when compared with estimates by the accelerometer.
IPAQ−STQ. The estimated mean ST was significantly lower for IPAQ (M = 303.8 minutes [163.4]) than for the STQ (M = 605.2 minutes [296.2]). There were no significant estimate differences among the stratified groups.