
The Effect of Radium-223 Therapy in Agent Orange-Related Prostate Carcinoma





Background: Radium-223 (Ra-223) radioisotope has been reported to increase median survival in bone metastatic prostate carcinoma. The addition of Ra-223 to abiraterone was associated with an increased risk of bone fractures. There has been no comprehensive data for using Ra-223 in veterans who were exposed to Agent Orange (AO+).
M ethods: We present a retrospective study of veterans with bone metastatic castration-resistant prostate cancer (CRPC) who received standard doses of Ra-223 and other sequential therapies at US Department of Veterans Affairs Pittsburgh Healthcare System in Pennsylvania from 2014 to 2018. Veterans were divided into 2 groups: those who were exposed to Agent Orange (AO+) and those who had no exposure (AO-). Time to study was calculated from the initiation of Ra-223. Time to skeletal-related events (SRE), progression of prostate specific antigen (PSA), bone metastasis, and alkaline phosphatase (ALP) were calculated in months using unpaired t test with 2-tailed P values. Median survival was calculated by Kaplan Meier R log-rank test.
Results: There were 34 veterans with bone metastatic CRPC: 17 veterans (50%) were AO+ and 17 veterans (50%) were AO-. The mean age of diagnosis of AO+ veterans was 62 years and 69 years ( P = .005) for AO- veterans (the mean Gleason score 8.2 and 8.0, respectively [ P = .71]). The median number of Ra-223 cycles was 6 (60%). Ten veterans received Ra-223 as first line (29%) and 24 veterans received Ra-223 later (71%). There were 12 SREs with median survival of 15 months. There was no difference in mean time to SRE between AO+ (8 veterans, 10.6 months) and AO- (4 veterans, 10.3 months) ( P = .93). The mean time to PSA progression for AO+ was 5.4 months and AO- was 6.8 months ( P = .28). Mean time to bone progression for AO+ was 7.6 months and AO- was 10.1 months ( P = .16). Mean time to ALP progression for AO+ and AO- was 6.3 months and 8.7 months, respectively ( P = .05). Twenty veterans (58%) had died. Median survival for Ra-223 first was 32 months and for Ra-223 later was 15 months ( P = .14; hazard ratio [HR] 0.48; 95% CI, 0.17- 1.3). Median survival for AO+ and AO- veterans was 12 months and 18 months, respectively ( P = .15; HR, 2.0; 95% CI, 0.77-5.0).
Conclusions: There was no statistical difference between AO+ and AO- veterans in terms of time to SRE, PSA, bone and ALP progression, even though there was a trend of shorter duration in AO+ veterans. There was no median survival difference between Ra-223 first vs Ra-223 later as well as between AO+ and AO- but there is a trend of worse survival in AO+ veterans.
Statistics
Time to study was calculated from the initiation of Ra-223 therapy. Time to skeletal-related events (SRE), progression of prostate specific antigen (PSA), bone metastasis, and alkaline phosphatase (ALP) were calculated in months, using unpaired t test with 2-tailed P value. Median survival was calculated in months by Kaplan Meier R log-rank test Definition).
Results
Forty-eight veterans with bone metastasis CRPC received Ra-223 therapy. Of those, 34 veterans were eligible for this retrospective study: 17 AO+ veterans and 17 AO- veterans. Mean age of diagnosis was 62 years (AO+) and 69 years (AO-) (P = .005). Mean Gleason score was 8.2 (AO+) and 8.0 (AO-) (P = .705). Veterans received initial therapy at diagnosis of prostate carcinoma, including radical prostatectomy (6 AO+ and 3 AO-), localized radiation therapy (3 AO+ and 5 AO-), and ADT (8 AO+ and 9 AO-) (Table 1).
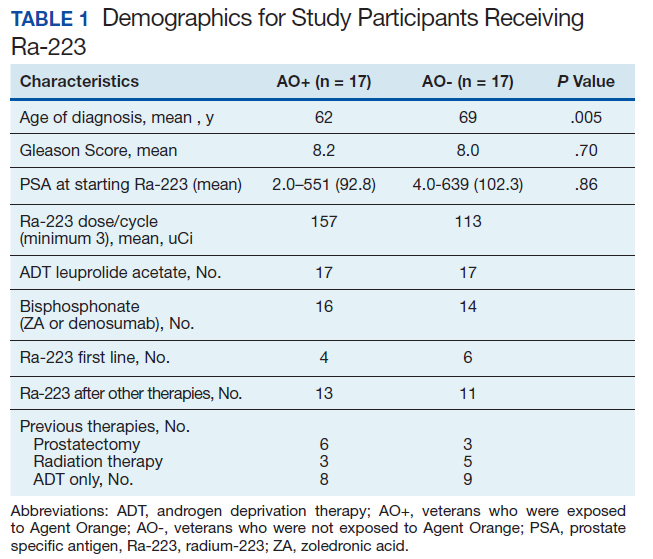
Mean PSA at the initiation of Ra-223 therapy for AO+ was 92.8 (range, 2-551) and for AO- was 102.3 (range, 4-639; P = .86). Mean Ra-223 dose per cycle for AO+ and AO- was 157 uCi and 113 uCi, respectively. All 34 veterans received ADT (leuprolide acetate), and 30 veterans (16 AO+ and 14 AO-) received bisphosphonates (zoledronic acid or denosumab). A total of 10 veterans (29%) received Ra-223 as a first-line therapy (4 AO+ and 6 AO-), and 24 veterans (71%) received Ra-223 after hormonal or chemotherapy (13 AO+ and 11 AO-).
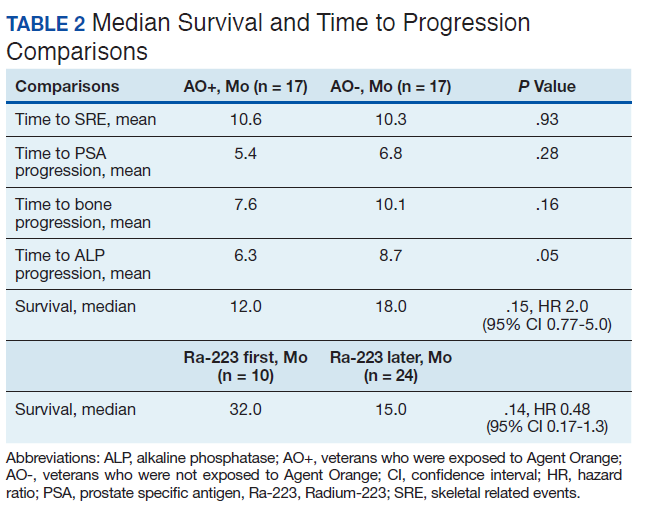
There were 12 SRE (8 AO+ and 4 AO-). Mean time to SRE for AO+ was 10.6 months and AO- was 10.3 months (P = .93). Three veterans received concurrent Ra-223 and abiraterone (participated in ERA 223 trial). Two AO+ veterans experienced SRE at 7 months and 11 months, respectively. Mean time to PSA progression for AO+ was 5.4 months and for AO- was 6.8 months (P = .28). Mean time to bone progression for AO+ and for AO- were 7.6 months and 10.1 months, respectively (P = .16). Mean time to ALP progression for AO+ and AO- were 6.3 months and 8.7 months, respectively (P = .05). (Table 2). The treatment pattern of AO+ and AO- is depicted on a swimmer plot (Figures 1 and 2).

Twenty veterans (58%) had died: 13 AO+ and 7 AO- veterans. Median survival for Ra-223 first and Ra-223 later was was 32 months and 15 months, respectively (P = .14; hazard ratio [HR], 0.48). Overall median survival for AO+ veterans and AO- veterans were 12 months and 18 months, respectively (P = .15; HR, 2.0) (Figures 3 and 4).

Discussions
There has been no reported VA study of using Ra-223 and other therapies (hormonal and chemotherapy) in veterans exposed to AO. This is the first retrospective study to compare the response and survival between AO+ and AO- veterans. Even though this study featured a small sample, it is interesting to note the difference between those 2 populations. There was 1 prior study in veterans with prostate carcinoma using radiotherapy (brachytherapy) in early-stage disease. Everly and colleagues reported that AO+ veterans were less likely to remain biochemically controlled compared with AO- and nonveteran patients with prostate carcinoma.4