Brown recluse spider bite? Consider this uniquely conservative treatment






An antihistamine and observation work as well—and often better—than more intensive therapies.
I decided to simply observe patients’ wounds for 7 to 10 days before performing debridement, advising patients to use an antihistamine to control symptoms during the waiting period. I took photographs to document clinical progression of wounds. In reviewing these photographs, I noted that the necrotic wounds stabilized immediately on starting an antihistamine—specifically, Benadryl, 5 mg/kg or 50 mg qid. After 7 to 10 days, I debrided the wounds, using fluorescein and a Woods lamp to guide the procedure. I found that tissue of doubtful viability survived if debridement was conservative and the patient had used an antihistamine (FIGURE 3).
FIGURE 3
Bite wound treatment: Observation for 7 to 10 days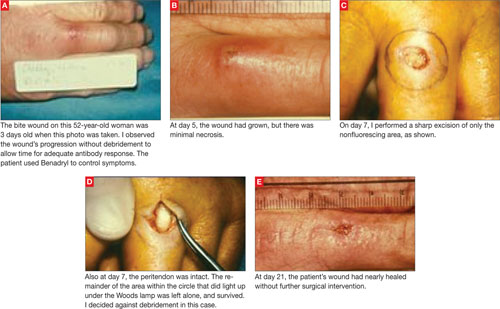
In reviewing phase 2 results in preparation for a presentation to the Southwestern Surgical Congress, I realized that debridement was rarely indicated. So, from 1981 to 1982, I relied less on surgery and more on conservative therapy. Patients got better simply with antihistamine therapy. Redness diminished very quickly once patients took the antihistamine, and pockets of purulent material drained on their own.
This approach also allowed antigen recognition to occur and seemed to prove the postulate of a less severe second bite. I saw 4 patients with proven “second set” spider bites (intact specimens were available) and all had an immediate inflammatory response and no subsequent necrosis. An 18-month-old patient with a bite below her right eye healed with Benadryl therapy alone (FIGURE 4).
FIGURE 4
Bite wound treatment: Antihistamine alone
Phase 4: Exclusive antihistamine therapy
Since 1982, I have treated more than 100 patients (myself included) with necrotic bite wounds from spiders and other insects. None have required operative debridement, and all have achieved much more acceptable cosmetic results using Benadryl therapy than with surgical therapy.
My encounter with a brown recluse. The bite I received was rather typical. I felt a sharp sting when outside working on the lawn. I looked down, saw nothing, and assumed I had run into a pin or small stick that was now not visible. For 3 days I noticed nothing unusual. On day 4, after showering I noticed a large amount of purulent material on the towel after drying my anterior left leg. On inspecting the area, I saw an area of necrosis approximately 6 × 6 cm with a central area oozing a purulent material. This appeared just like the necrotic insect bites I had treated with antihistamines, so I started myself on that regimen. The redness cleared up in 2 days and the wound healed completely in 10 days without antibiotics. A 3 × 3 mm circular scar remained; I lost none of the surrounding marginal skin.
Further evidence of less severe second bites. Another physician—my coauthor on the presentation to the Southwestern Surgical Congress—was bitten at age 12 by an unidentified insect, resulting in a large necrotic wound on his thigh. The lesion, reportedly 10 to 12 cm in diameter, healed with topical treatment only. After our joint report in 1982, a brown recluse spider bit him on the abdomen while he was working in the yard. He captured the spider and verified its genus and species. Guessing that the bite he received as a 12 year old was also from a brown recluse, he decided to wait and see if he had a “second set” reaction to the bite. He had an immediate inflammatory reaction, no skin necrosis, and the entire area returned to normal in 3 days. His experience became the fifth “second set” spider bite reaction in our series.
Another dramatic experience. One 22-year-old woman’s experience is worth a longer discussion. She visited her physician because 4 small areas of necrosis on her lower abdomen and chest had lasted several days and were getting worse. He assumed these were small abscesses and treated her with antibiotics. The lesions slowly enlarged to become 6 to 8 cm in diameter, and the physician hospitalized her for intravenous (IV) antibiotic therapy.
When the patient worsened after 2 days of IV antibiotics and incision and drainage, I was called to examine her for possible surgical debridement. I thought the lesions were necrotic insect bites and recommended starting Benadryl, 50 mg qid. She improved remarkably over the next 24 hours, her wounds decreasing in size by 50%. She was discharged from the hospital and, against my advice, the Benadryl was stopped. Within 48 hours the area of inflammation around the wounds had doubled in size. She was readmitted and given Benadryl. Again she improved remarkably in 24 hours. The purulent discharge was sent for culture, which grew an organism resistant to all of her previous antibiotics. She healed uneventfully in 10 days on antihistamines, and without antibiotics. This is typical in my experience. Antibiotics have seldom proved useful, and culture results are generally confusing.