Deep Space Infections of the Neck: Considerations in Diagnosis and Management






Despite the decreased incidence of deep space neck infections since the advent of antibiotics, preventive healthcare, and improved hygiene, this condition still carries a high rate of complications and morbidity.
Pathophysiology and Microbiology
Deep space neck infections often begin as cellulitis adjacent to the primary source of infection and may progress to abscess formation. Abscess may also directly arise from perforation of the lymph node capsule. Fascial layers initially confine both cellulitis and abscess. Further spread tends to involve adjacent or communicating compartments.15,16
In the pre-antibiotic era, the most common organism associated with deep space neck infection was Staphylococcus aureus. Now, due to drug resistance and microbial flora change, these infections are most commonly associated with aerobic streptococcal species and nonstreptococcal anaerobes.4Streptococcus viridans is the predominant organism in adult neck infection (43.7%), with Klebsiella pneumoniae slightly more prevalent in diabetic patients (56.1%).8 The standard of care is to presume polymicrobial infection and to provide empiric coverage for both aerobic and anaerobic infection. Any condition that reduces the blood supply to an affected area (eg, trauma, foreign body, malignancy, surgery, edema, shock, vascular disease) creates a hypoxic environment—ideal for anaerobic infection.2
,Anatomy
For successful management of patients with deep space neck infections, the provider must have a working knowledge of neck anatomy, common etiologies, typical presentations, and potential complications.3 Several classification systems are currently used to describe specific deep neck spaces. Essentially, there are three major clinically important spaces between the deep cervical fascia: the parapharyngeal, submental and submandibular, and retropharyngeal spaces.
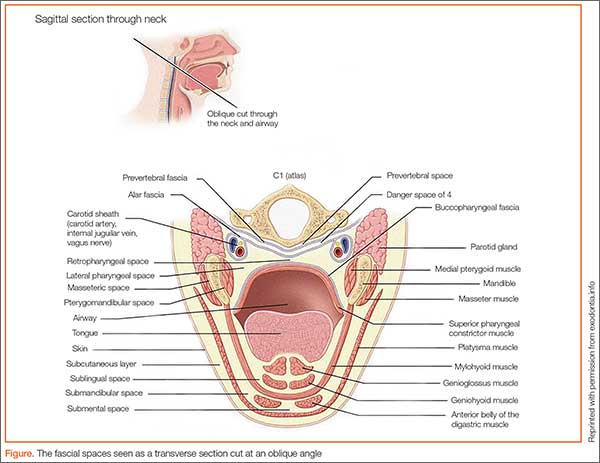
The parapharyngeal (or lateral pharyngeal), located in the upper neck, extends superior to the hyoid bone. The parotid gland and mandible (lateral) are located in this space and are bound by the pretracheal fascia of the visceral compartment and the superficial fascia (which appears as an inverted cone). The submental and submandibular triangles contain the second space, located between the mucosa of the floor of the mouth and superficial layer of the deep fascia. Lastly, the retropharyngeal space running from the base of the skull to the posterior mediastinumis is bordered posteriorly by the prevertebral fascia and anteriorly by the posterior portion of the pretracheal fascia.4,15,16
A knowledge of cervical fascia anatomy is critical to understanding the likely source, predicting the extent of the progression of infection as well as aiding in the choice of medical versus surgical treatment.4 From a purely anatomic standpoint, deep space neck infections follow the path of least resistance, penetrating the nearest and thinnest cortical bone and tracking along the fascial planes in the neck and face.8 The tough connective tissue of the deep cervical fascia in the neck, which is divided into superficial, middle, and deep layers, prevents the egress of pus toward the skin. As a result, infections will alternatively descend toward the mediastinum, ascend to the lateral pharynx and masticator spaces, or expand to the point of airway obstruction. (See the Figure for a sagittal illustration of the fascial spaces.)
Ludwig’s Angina
While the aim of this article is for comprehensive knowledge of deep space neck infections, it is worth turning attention to one condition that has high name recognition and is representative of the discussion. Ludwig’s angina was first described in 1836 by German physician Wilhelm Frederick von Ludwig as a rapidly and frequently fatal progressive gangrenous cellulitis and edema of the soft tissues of the neck and floor of the mouth, which he considered a “morbid entity.”17
Although the term “Ludwig’s” is often loosely applied to deep space neck infections, it should be limited to those infections which are bilateral and involve the submandibular space (including both the sublingual and submylohyoid spaces). Prior to the advent of antibiotics, swelling frequently led to respiratory obstruction and death; thus, the term angina was added to the description (angina coming from the word angere, meaning “to strangle.”4,18,19
Diagnosis
Physical Examination
When evaluating a patient with a suspected deep space neck infection, an orderly evaluation should be conducted following the basic principles of a thorough physical examination, including visualization, palpation, and percussion.4 Careful examination alone may obviate the need for imaging prior to consultation and result in decreased time to surgical intervention.
Vital Signs. Patients with deep space neck infections are often quite ill, some with associated shock. As is the case with all presentations to the ED, the physical examination should always begin by documenting the patient’s blood pressure, pulse, temperature, peripheral perfusion by assessment of capillary refill time, skin temperature, degree of moisture/dryness, and oxygen saturation.
General Observations. Note the overall level of patient comfort and position. A seated patient leaning forward in the sniffing position is an ominous sign, and placing such a patient supine may lead to complete airway collapse.