Stridor in the Pediatric Patient





Epiglottitis
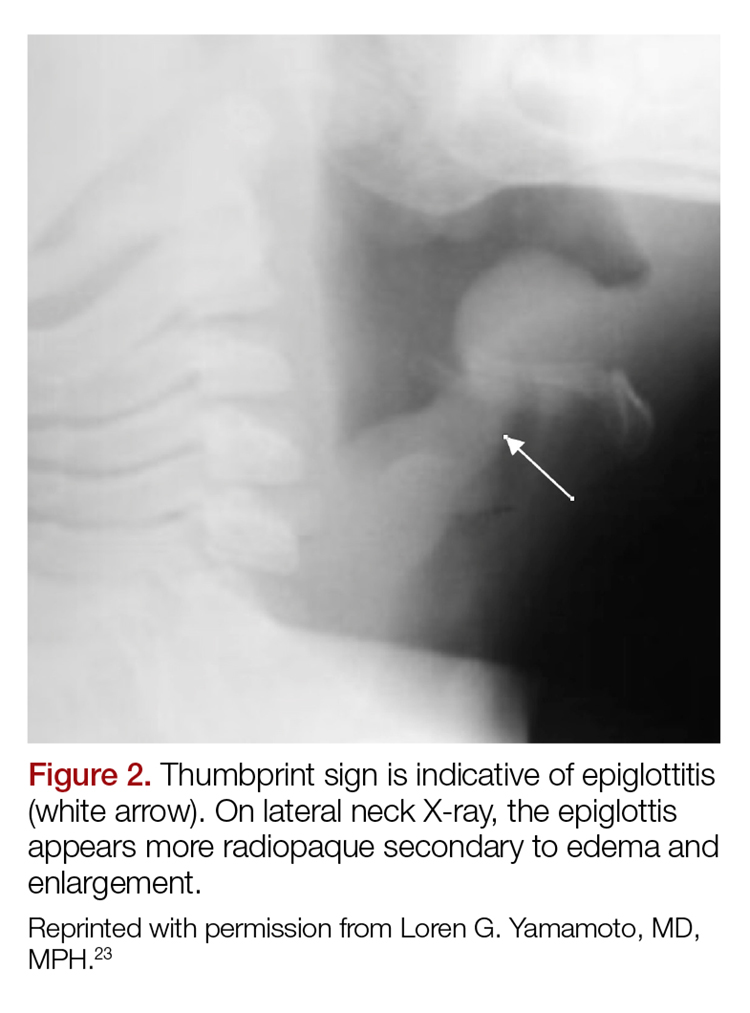
Epiglottitis is edema of the epiglottis, most commonly secondary to bacterial infection. The epidemiology of epiglottitis has changed dramatically since widespread immunization for H. influenza with a significantly decreased incidence and change in the average age of presentation to 14.6 years (previously 5.6 years).7 The clinical course begins with sore throat, dysphonia, refusal to eat and progressive difficulty handling secretions with eventual drooling, stridor, tripoding, and toxic appearance. Epiglottitis can be differentiated from croup and bacterial tracheitis because presentation typically lacks a cough.7,10,11 Diagnosis is made either by direct visualization of the epiglottis or a lateral neck X-ray showing a ‘thumb print’ sign (Figure 2).12 Emergency department treatment is similar to the management of the child with a partial foreign body occlusion and focuses on maintaining the airway and minimizing anything that agitates the patient. Intravenous (IV) antibiotic coverage is similar to bacterial tracheitis (third-generation cephalosporin or a beta-lactamase resistant penicillin).
Retropharyngeal Abscess
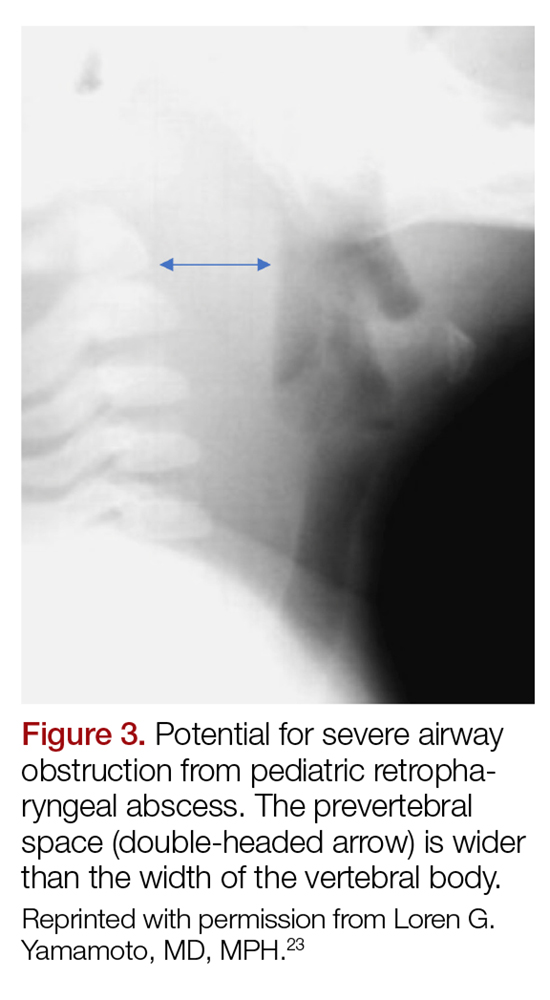
The most common chief complaint of retropharyngeal abscess (RPA) is neck pain (38%) with fever. As such, it can clinically be mistaken for meningitis on initial presentation. Retropharyngeal abscess will present rarely with either stridor or associated respiratory distress, and it can also mimic croup on initial presentation. Physical examination findings which differentiate this entity include limited or painful neck extension (45%), torticollis (36.5%), and to a lesser extent limitation of neck flexion (12.5%).13 The median age at diagnosis is 36 months with 75% of patients less than 5 years. Typical presentation is insidious with fever and URI symptoms preceding onset. Diagnosis can be made with a lateral neck X-ray showing widening of the prevertebral space (Figure 3), but the gold standard diagnostic study is a computed tomography with contrast.14 Management is IV antibiotics covering aerobic and anaerobic bacteria (eg, ampicillin-sulbactam) ± surgical intervention.
Caustic Ingestion
Caustic ingestion is most commonly accidental and seen in children aged 12 months to 2 years. However, with recent fads, such as the “Tide Pod challenge” teenagers are also at risk. Airway compromise and stridor are secondary to mucosal injury and edema. Oral injury is not always a useful marker for significant distal injury. A complete evaluation of the upper airway and digestive tract within 48 hours after known/suspected caustic ingestion is recommended to assess full extent of damage.15
Chronic Differentials
Laryngomalacia
Laryngomalacia is a congenital weakness of laryngeal tissues, and it is the most common cause of both chronic stridor and neonatal stridor. It is characterized by progressive worsening of symptoms with crying/feeding and supine positioning. Diagnosis is made by bronchoscopy and management is conservative unless there are life threatening apneic or cyanotic events.7
Rings/Slings
There are many anatomic structures with the potential to cause extrinsic airway compression which present with stridor. This type of stridor is often biphasic. Examples include innominate artery compression, double aortic arch, aberrant subclavian artery, and pulmonary artery sling.7
Stridor presenting in children with a history of prematurity or prolonged intubation should raise concern for subglottic and tracheal stenosis.16