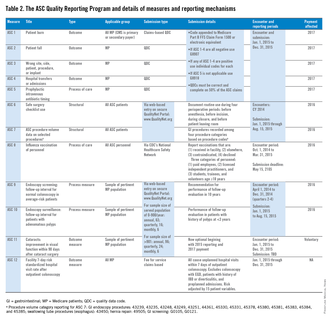
Quality Improvement for the Ambulatory Surgery Center





The ASC Quality Reporting Program began in 2012 with five measures developed and owned by the Ambulatory Surgery Center Association. They were generic and applicable to most surgical environments, but minimally so to gastrointestinal endoscopy. During 2014, the ASC Quality Reporting Program will require ASCs to report on 11 perioperative measures (ASC 1-11) to avoid payment decrements for 2016 (Table 2).11 Among these measures, measures 2-4 and 6-10 are pertinent to gastrointestinal endoscopy units. ASC 1 through ASC 5 are reported via claims-based quality data codes (defined for each measure), ASC 8 (influenza vaccination of personnel) is reported on the CDC’s National Healthcare Safety Network, and the other measures are submitted via web-based entry on the secure quality net portal.
The quality improvement process
Many practice changes can be addressed administratively, but substantive improvement or redesign in care processes is facilitated by formal improvement projects, defined by assembling a team of responsible individuals who define a transparent plan with clearly delineated goals, use of established techniques, and a time line. Improvement teams should include both staff and managers with responsibility for the process or outcome being addressed, and individuals with skills and experience with database queries, data acquisition, statistical assessment, and process control charting.
Most major quality improvement methodologies use steps analogous to those of the basic plan, do, study, act method, which uses cycles of planning, pilot testing, analysis of test results and lessons learned, followed by full adoption of new processes into practice, vs. repeated plan, do, study, act method cycles. This approach is used commonly to identify rapid stepwise improvements when time and resources are limited.
Commonly used quality-assurance practices
Numerous well-established practices in health care provide oversight and assurance regarding the quality of care delivered by an individual or a practice (Table 3). They vary greatly in rigor and frequency of use. Some are mandated and several others can be adapted easily for use by independent ambulatory centers.

Accreditation, or analogous state health department certification, is required by the CMS to gain so-called deemed status, by which a facility is deemed to be in compliance with CMS’s regulatory standards, as delineated in the Conditions for Participation (available at: https://www.cms.gov/Regulations-and-Guidance/Legislation/CFCsAndCoPs/index.html?redirect=/CFCsAndCoPs/06_Hospitals.asp). Deemed status is required to bill for service to CMS clients. Accreditation, therefore, encompasses numerous other expectations, including credentialing of professional staff at initial appointment and biannual privileging thereafter, monitoring of adverse and sentinel events, routine assessment of patient satisfaction, and use of ongoing quality improvement programs pertinent to the services delivered. Despite their seemingly burdensome nature, these processes should be embraced as opportunities for a facility to unapologetically assess the quality of their providers, outcomes for their patients, and overall practice performance.
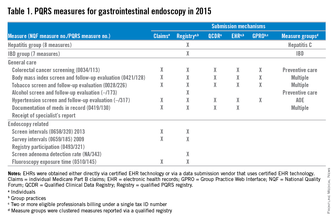
Benchmarking is a method for comparing one’s performance and outcomes against those from similar individuals or institutions. In contrast to audit-feedback programs, external benchmarking sometimes is referred to as participation in a registry that typically provides comparison against aggregate data from many groups. Risk adjustment for differences in populations and services can enable comparison between disparate groups. A prime motivation for participating in national registries for endoscopy or other focused practice areas within clinical gastroenterology (hepatitis and inflammatory bowel disease [IBD] care) is to facilitate automated submission of performance data on quality measures to CMS, for which entry of some measures is required to be completed through certified registries. As these mechanisms evolve, registry participation will become another de facto necessity for most practices.
The GI Quality Improvement Consortium is a nonprofit national registry collaboratively established and wholly owned by the American Society for Gastrointestinal Endoscopy and the ACG, and built and run by Quintiles Outcomes Inc. The program provides comparative results on numerous unit-wide and physician-specific quality measures pertaining to endoscopy (colonoscopy and esophagogastroduodenoscopy; endoscopic retrograde cholangiopancreatography pending). The measures of interest are submitted electronically after either manual abstraction or automated retrieval from an electronic endoscopic report generator. Registered physicians can report individual PQRS measures and measure groups via the Outcome PQRS registry, which generally provides greater success in participation, compared with submission via the claims-based mechanism. The GI Quality Improvement Consortium also provides the measures and results necessary for providers to complete an American Board of Internal Medicine self-directed Practice Improvement Module (PIM) for either colonoscopy or esophagogastroduodenoscopy.
Built in partnership with the Health Care Incentives Improvement Institute, the AGA Digestive Health Recognition Program (DHRP) was designed to provide quality reporting that is familiar to payers, and has been successful in other specialties. In addition, the DHRP supports the submission of data to the CMS to meet requirements for the PQRS, and avoid reimbursement penalties for nonparticipation. In the DHRP, 30 consecutive Medicare patients are used for data extraction and submission using a web-based tool. DHRP currently is available for IBD and hepatitis C practices, and is linked to Bridges to Excellence recognition, a program of the Healthcare Incentives Improvement Institute, designed to recognize and reward clinicians who deliver superior patient care. The DHRP also supplies providers with the measures and results necessary to complete an ABIM self-directed Practice Improvement Module for either IBD or hepatitis C. A module is in development for colon cancer prevention (available at: https://www.gastro.org/practice/quality-initiatives/aga-digestive-health-recognition-program).