Management of HIV/AIDS





With the advances in antiretroviral therapy and increased life expectancy of
patients with HIV infection, the emergency physician must also consider noninfectious pathologies in the differential diagnosis.
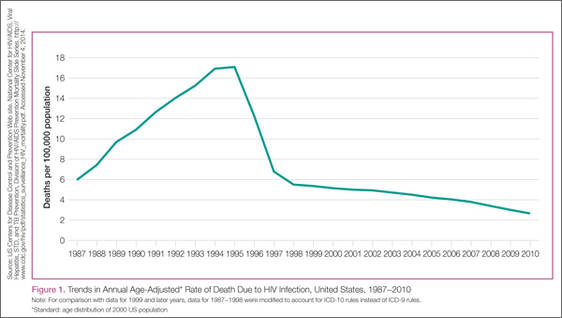
The US Centers for Disease Control and Prevention (CDC) estimates that 1.1 million people in the United States are living with HIV, with one in six of those individuals being unaware of their infection. Despite education and prevention efforts, each year approximately 50,000 people are newly infected. Less than 40% of people living with HIV are in regular care, and less than 25% are on antiretroviral therapy with a resultant suppressed viral load.1 In 2010, 15,529 of these individuals died.2 Although there have been great advances in the fight against HIV over the past several decades, the infection continues to be a major public health issue.
Changing Landscape
Highly active antiretroviral therapy (HAART) has decreased mortality associated with opportunistic infections, resulting in substantial increases in life expectancy.3-5 In one single-center study conducted from 2000 to 2005, admissions due to opportunistic infections in HIV-positive individuals decreased, while those due to renal, oncologic, and psychiatric comorbidities as well as medication adverse events increased.6
Routine Testing in the ED
In 2006, the CDC revised the guidelines for HIV testing in healthcare settings.7 The new recommendations included opt-out screening as an important strategy to assure HIV testing as a routine part of medical care. In April 2013, the US Preventive Services Task Force reinforced this message by issuing a grade A recommendation that clinicians test for HIV infection all adolescents and adults aged 15 to 65 years, including all pregnant women, as well as younger adolescents and older adults with risk factors for infection.
Subsequently, the number of EDs conducting HIV testing has substantially increased. Screening programs in the ED are a public health service and do result in important changes in clinical management of certain patients, but they can also present challenges. The institution of screening policies, such as opt-in versus opt-out testing, can be contentious and logistically difficult. A balanced presentation of these issues appears in the July 2011 issue of Annals of Emergency Medicine, which is focused on HIV screening in the ED.8
Fourth Generation HIV testing
Detecting HIV RNA is an expensive and laborious process, so screening and testing programs had relied on antibody-based assays. Until 2009, the third-generation antibody HIV assays available in the United States were effective in detecting chronic HIV infections but could not detect acute HIV infections (the period of time during which an individual is infected but has not yet produced antibodies). In June 2010, the US Food and Drug Administration approved fourth-generation tests that detect both antibodies and the p24 HIV antigen. The p24 antigen, a highly conserved capsid protein on the virus, is detectable early after infection and is associated with the initial burst of virus replication after infection. Levels of p24 start to drop approximately one month after infection, just at the point when antibody levels are usually detectable. Thus, the fourth-generation tests offer a substantial improvement in detection of early HIV infection. Estimates of the sensitivity of fourth-generation tests for early HIV infection vary. In two US studies, stored blood samples from people with acute infection were tested. Each sample tested positive for HIV RNA but negative for HIV antibodies. In the first study, 48 of 58 samples (82.7%) were correctly identified, whereas in the second study, 13 of 21 (61.9%) had a correct positive result.9 A German evaluation of 11 different fourth-generation tests found that the most sensitive test was positive 6.2 days after detection of RNA, while the least effective test identified infection 10.7 days later, a performance similar to that seen with third-generation tests.10