Intimate partner violence: How you can help female survivors





ABSTRACTIntimate partner violence (IPV) is a prevalent, complex, and challenging women’s health problem associated with a number of negative medical, reproductive, and mental health conditions. When clinicians bring up the topic with their patients, patients are more likely to disclose. Supportive counseling and referrals are associated with improved safety and health.
KEY POINTS
- Many victims of IPV will not present with injuries but may have medical or mental health issues related to their IPV experiences.
- Addressing IPV with female patients not only results in increased identification of survivors but is also associated with cognitive and emotional benefits.
- IPV information and resources should be provided to all women, regardless of IPV disclosure.
- Clinicians should respond to a patient’s IPV disclosure with validation, support, respect, and information.
- Clinicians must respect patients’ autonomy, as they are the ones who best understand their situation and know what they need. In some cases, leaving an abusive relationship can be more dangerous than staying.
Just asking may be an intervention
Qualitative studies have suggested that just the act of asking about IPV in a nonjudgmental and compassionate manner is helpful to women experiencing IPV.35,37 Doing so not only helps women recognize the abuse, but also begins to decrease their sense of isolation and increase their awareness of helpful resources. It also gives the patient a sense that the clinician cares about her situation.35 As a result, experts have begun to recommend that health clinicians view asking about IPV not merely as a screening tool, but as a potentially therapeutic intervention in and of itself.35,37,38
HOW TO HELP
What to do when a woman discloses IPV
Female survivors, advocates, and health care clinicians who care for abused women suggest responding to a positive disclosure of IPV by providing the following:
Validation. The IPV perpetrator will often attempt to justify the violence and abuse by shifting some of the blame or responsibility for the violence onto the victim. This “brainwashing” leads to self-blame and a diminished sense of self-worth. However, clinicians can help reverse this mindset by acknowledging the woman’s disclosure and emphasizing that she did not deserve the abuse or violence. An example of such a statement is, “I am so very sorry that you went through that with your partner. You definitely did not deserve that. No one should ever be hurt by or afraid of the people who are supposed to love them.” Providing validation helps women recognize that the violence was a problem they did not deserve.38,39
Support. Women who have experienced IPV appreciate feeling supported and cared for by their health care clinician. Even if the patient is not ready to take any definitive action regarding her relationship or situation, knowing that her clinician and the health care setting are resources and sources of support is both comforting and empowering.35,40 Clinicians can communicate this support by stating, “I want you to know that whatever happens and whatever you decide, we are here for you.”
Respect for autonomy. Women experiencing IPV best understand their own situation and its various complexities and so they know best what they can do, cannot do, or need to do. As such, clinicians must respect a woman’s autonomy and preserve her ability to express her own needs and desires and make her own decisions. Prescribing a plan of action or giving commands to IPV victims could further perpetuate their sense of disempowerment and lack of control over their life.
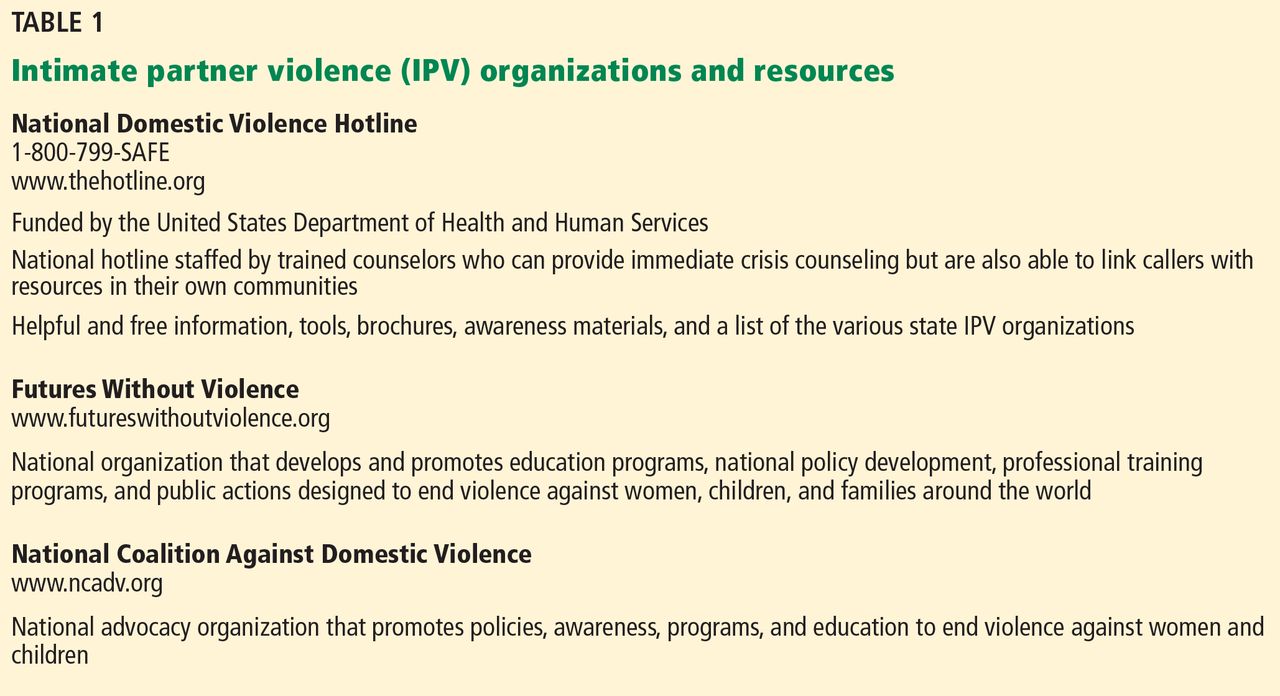
Information. Providing referral information or hotline numbers to community domestic violence programs is helpful. However, not all women feel safe or comfortable taking printed brochures or written information with them because their abusive partner may find it. Thus, clinicians should ask if the patient can take the information safely or offer to write the numbers down without labeling them if she is afraid. The National Domestic Violence hotline is a 24-hour toll-free resource that will help women locate and contact shelters and other support services in their own community. The number, 1-800-799-SAFE (7233), is easy to memorize and thus is an easy resource to pass along quickly and safely. Other national organizations such as Futures Without Violence (formerly known as the Family Violence Prevention Fund) and the National Coalition Against Violence also provide links to local resources (Table 1).
Safety planning. Discussing the need for a safety plan will help the patient prepare for future abusive episodes. Even women who report that they are no longer in an abusive relationship should be asked about their current safety needs and concerns because they often remain in contact with abusive partners even after a relationship has ended.
When discussing safety planning, clinicians should ask the woman if she is currently safe or if she needs shelter. If she intends to return to or is still in contact with her batterer, ask if she has a plan for what to do or how to escape if the violence occurs again. Advise the patient to:
- Hide money so that she can leave quickly
- Make copies of birth certificates, immunization records, Social Security Number, and other important documents and keep them hidden and accessible
- Make a spare car key
- Have a list of hotline numbers
- Develop a code with friends, family, and neighbors that will let them know she needs immediate help.
Studies show that discussing safety-promoting behaviors increases the number of them that are used by IPV victims.41 A detailed list that can be shared with patients is provided in the patient information page that accompanies this article.42 Examples of personalized safety plans are available from the National Center on Domestic and Sexual Violence at its website, www.ncdsv.org/images/NCDSV_DVSafetyPlan_updated2013.pdf.
Danger assessment. Several researchers have examined potential risk factors associated with increased risk of homicide.43 Table 2 lists some of the characteristics associated with an increased risk of homicide in IPV situations.42 From this work, a danger assessment tool and scoring system has been developed. This tool and training on how to use it are available for free at www.dangerassessment.org. Although there are currently no outcome data on the benefits or risks of using this instrument, its objective is to increase women’s awareness of their danger level and individualize their safety counseling.
Proper documentation. Victim advocates and lawyers working on behalf of IPV victims emphasize that documentation by a medical provider can help a woman with her legal case. This documentation should be clear, legible, and as detailed as possible. These details should include a patient’s own words set off by quotation marks, a description or body map illustrating associated injuries or physical signs corroborating the violence, and a description of the patient’s demeanor or signs of emotion. Clinicians should avoid legal terms such as “alleges” or “alleged perpetrator” and should either define or avoid abbreviations that may be considered ambiguous in a legal proceeding (eg, clinicians should write out the words “domestic violence” or “intimate partner violence” rather than using “DV” or “IPV”).44 Most states have passed laws that prevent insurance companies from discriminating against IPV victims; insurance companies can no longer deny women coverage for seeking care related to IPV.45