Depression and coronary heart disease: Association and implications for treatment





ABSTRACT
Growing evidence indicates that depression is an important primary and secondary risk factor for coronary heart disease (CHD). Depression is quite common among patients with CHD: prevalence estimates are 14% or higher, and an additional 20% of patients have subclinical or minor depression. This review summarizes evidence that depression is a risk factor for cardiac events in patients with established CHD, suggests potential mechanisms underlying the relationship between depression and adverse cardiac outcomes, and provides evidence for the efficacy of exercise in improving both depression and clinical outcomes in depressed patients with CHD.
STUDIES OF DEPRESSION TREATMENT IN CARDIAC PATIENTS
Successful treatments for depression in patients with CHD may have the potential to improve not only quality of life but also cardiovascular and physical health. Several treatments for depression exist for use in the general population, such as antidepressant medication or psychotherapy.41 However, only three studies have tested the efficacy of these treatments in patients with CHD: SADHART, ENRICHD, and CREATE.42–44
SADHART (Sertraline Antidepressant Heart Attack Randomized Trial) was a safety and efficacy evaluation of antidepressant medication in patients with MDD and a recent MI or unstable angina.42 It showed only modest differences in reductions in depressive symptoms between sertraline recipients and placebo recipients, and it lacked statistical power to examine the impact of treatment on hard clinical end points.
ENRICHD (Enhancing Recovery in Coronary Heart Disease Patients) assessed the effect of psychosocial treatment on survival among more than than 2,400 post-MI patients.43 Although this trial found that cognitive behavior therapy resulted in significant, albeit small, improvements in depressive symptoms compared with usual care, it failed to demonstrate that treating depression and low social support was associated with increased survival.
CREATE (Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy), a recent placebo-controlled trial, assessed the value of antidepressant medication and clinical management in patients with CHD.44 The study’s 284 patients, all of whom had CHD as well as MDD and a HAM-D score of 20 or greater, underwent two separate randomizations: (1) to 12 weeks of interpersonal therapy plus clinical management or 12 weeks of clinical management alone, and (2) to 12 weeks of citalopram therapy or matching placebo. There was no difference between interpersonal therapy and clinical management alone; however, citalopram was superior to placebo in reducing HAM-D scores and demonstrated better remission rates (35.9% with citalopram vs 22.5% with placebo). The same therapists who provided interpersonal therapy also performed the clinical management, so it could be argued that this was why additional interpersonal therapist time did not result in greater reductions in depressive symptoms than did clinical management alone. Furthermore, this study did not examine the effects of depression therapy on clinical outcomes.
EXERCISE AS A TREATMENT FOR DEPRESSION
There is growing evidence that exercise may be an effective treatment for depression.45 Most of the existing studies of exercise for depression have focused on aerobic exercise.
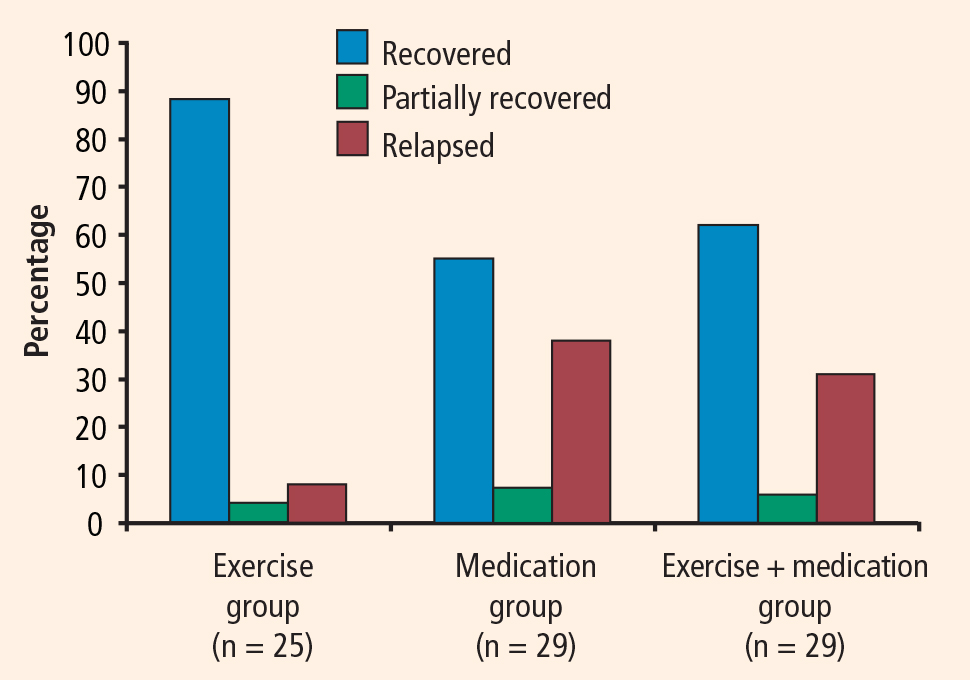
In the relatively large SMILE study (Standard Medical Intervention and Long-term Exercise),46 conducted at Duke University, 156 adult noncardiac patients with MDD were randomized to 4 months of treatment with supervised aerobic exercise, antidepressant medication (sertraline), or a combination of exercise and medication. Although antidepressant medication was associated with faster reductions in depression in the first 4 weeks of treatment among mildly depressed patients, exercise was as effective as antidepressant medication in treating depression by the end of the 16-week intervention for all participants.
Exercise generally is considered safe for most patients with stable CHD.48 Some studies of exercise treatments for patients with CHD have tracked depressive symptoms and thus have provided insight into the potential efficacy of exercise as a treatment for depression in this population. Although most of these studies have reported significant improvements in depression after completion of an exercise program, many have had important methodologic limitations, including absence of a control group. In one of the few controlled studies in this area, Stern et al49 randomized 106 men who had a recent acute MI and elevated depression, anxiety, or low fitness to 12 weeks of exercise training, group therapy, or usual care (control). At 1-year follow-up, subjects in both the exercise and counseling groups showed improvements in depression relative to controls.
EFFECT OF EXERCISE ON CARDIOVASCULAR RISK FACTORS AND OUTCOMES
Exercise is a particularly promising intervention for depression in patients with CHD because it has well-documented cardiovascular benefits. In addition to the well-established role of exercise interventions in primary prevention, such interventions have been shown to improve outcomes for patients with CHD.50
Jolliffe et al conducted a meta-analysis comparing exercise-only interventions, comprehensive rehabilitation (including educational and behavioral components such as dietary changes and stress reduction in addition to exercise), and usual care.51 Exercise-only interventions were associated with reductions in both all-cause and cardiac mortality relative to usual care. Comprehensive rehabilitation, on the other hand, was not associated with statistically significant reductions in all-cause mortality relative to usual care, but it was associated with a decreased risk for cardiac mortality, to a slightly lesser extent than exercise-only interventions.
The evidence that exercise affects depression, CHD risk factors, and CHD outcomes suggests that exercise is a particularly promising intervention for depression in this population.
UPBEAT trial promises further insight
A new Duke University study known as UPBEAT (Understanding Prognostic Benefits of Exercise and Antidepressant Treatment) is randomizing 200 patients with elevated depressive symptoms to exercise, antidepressant therapy (sertraline), or placebo for 4 months.53 A variety of “biomarkers” of risk are being assessed, including measures of heart rate variability, vascular function, inflammation, and platelet aggregation. Results of this 5-year trial should be available by 2011.