Depression and coronary heart disease: Association and implications for treatment





ABSTRACT
Growing evidence indicates that depression is an important primary and secondary risk factor for coronary heart disease (CHD). Depression is quite common among patients with CHD: prevalence estimates are 14% or higher, and an additional 20% of patients have subclinical or minor depression. This review summarizes evidence that depression is a risk factor for cardiac events in patients with established CHD, suggests potential mechanisms underlying the relationship between depression and adverse cardiac outcomes, and provides evidence for the efficacy of exercise in improving both depression and clinical outcomes in depressed patients with CHD.
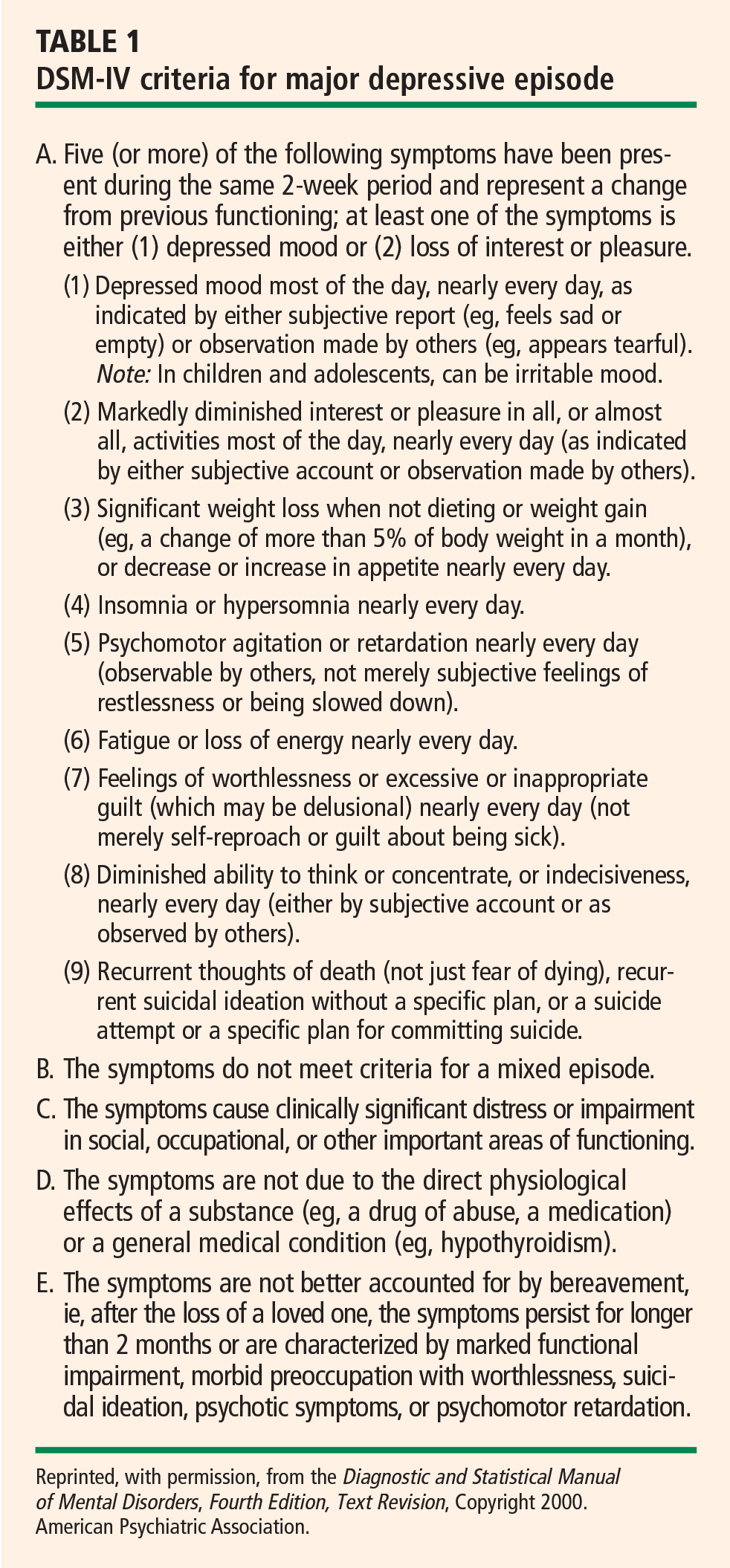
Minor depressive disorder (mDD) is not an official DSM-IV diagnosis but is used for research purposes; it is similar to MDD in duration but requires that only two to four symptoms be present.
EPIDEMIOLOGY OF DEPRESSION
Depression is a widespread and often chronic condition. Lifetime prevalence estimates for MDD are approximately 15% to 20%;2,3 1-year prevalence estimates are 5% to 10%;2,4 and point prevalence estimates range from 4% to 7%.3,5 Moreover, MDD is characterized by high rates of relapse: 22% to 50% of patients suffer recurrent episodes within 6 months after recovery.6
Women are twice as likely as men to be diagnosed with MDD, with lifetime prevalence rates of 10% to 25% in women versus 5% to 12% in men.1
Although rates of depression do not appear to increase with age, MDD often goes undertreated in older adults3 and in cardiac patients.7
DIAGNOSING AND ASSESSING DEPRESSION
The gold standard for diagnosing MDD is a clinical interview. Commonly used instruments include the Diagnostic Interview Schedule8 and the Composite International Diagnostic Interview.9 The Structured Clinical Interview for DSM-IV Axis I Disorders10 and the Schedule for Affective Disorders and Schizophrenia11 are frequently used semistructured interviews.
The most common clinical instruments for assessing the severity of depressive symptoms are the Hamilton Rating Scale for Depression (HAM-D),12 which is a clinician-rated scale, and various psychometric questionnaires, including the Beck Depression Inventory (BDI)13,14 and the Center for Epidemiological Studies Depression Scale (CES-D).15
THE DEPRESSION–HEART DISEASE LINK
Depression as a primary risk factor
Depression as a secondary risk factor
Depression is an even stronger risk factor for cardiac events in patients with established CHD. Point estimates range from 14% to as high as 47%, with higher rates in patients with unstable angina and in patients awaiting coronary artery bypass graft (CABG) surgery; an additional 20% of patients exhibit elevated depressive symptoms or minor depression (mDD).19–25
Prospective studies have shown that depression increases the risk for death or nonfatal cardiac events approximately 2.5-fold in patients with CHD. For instance, Frasure-Smith et al followed 896 patients with a recent acute MI and found that the presence of depressive symptoms as indicated by an elevated BDI score was a significant predictor of cardiac mortality after controlling for multivariate predictors of mortality (odds ratio [OR] = 3.29 for women and 3.05 for men).26
Two recent meta-analyses confirmed the association between depression and adverse clinical outcomes in patients with CHD.27,28 For example, van Melle et al reported that post-MI depression was associated with a 2- to 2.5-fold increase in the risk of adverse health outcomes.28 In this analysis, depression’s effect on cardiac mortality and all-cause mortality was especially pronounced in older studies (before 1992) (OR = 3.2) compared with more recent studies (after 1992) (OR = 2.01).28
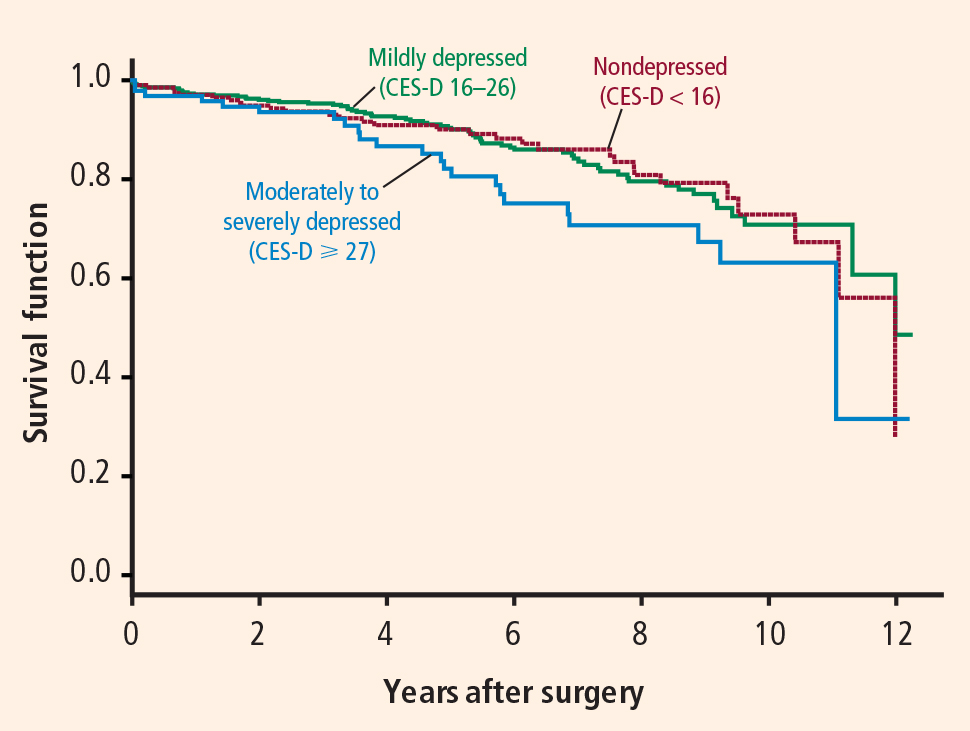
Duke University researchers have conducted several prospective studies in various cardiac populations.29–31 Barefoot et al assessed 1,250 patients with documented CHD using the Zung Self-Rating Depression Scale at the time of diagnostic coronary angiography and followed them for up to 19.4 years.29 Results showed that patients with moderate to severe depression were at 69% greater risk for cardiac death and 78% greater risk for all-cause death than were their nondepressed counterparts.
We also recently reported results from a prospective study that followed 204 patients with heart failure over a median interval of 3 years.31 Clinically significant symptoms of depression (BDI score ≥ 10) were associated with a hazard ratio of 1.56 (95% CI, 1.07 to 2.29) for the combined end point of death or cardiovascular hospitalization. These observations included adjustment for plasma NT-proBNP level, ejection fraction, and other established risk factors, suggesting that heightened risk of adverse clinical outcomes associated with depressive symptoms is not simply a reflection of the severity of heart failure.
In summary, a number of observational studies have demonstrated that depression is associated with increased risk of morbidity and mortality both in healthy populations and in a variety of populations with established cardiac disease.
BIOBEHAVIORAL MECHANISMS LINKING DEPRESSION AND CHD
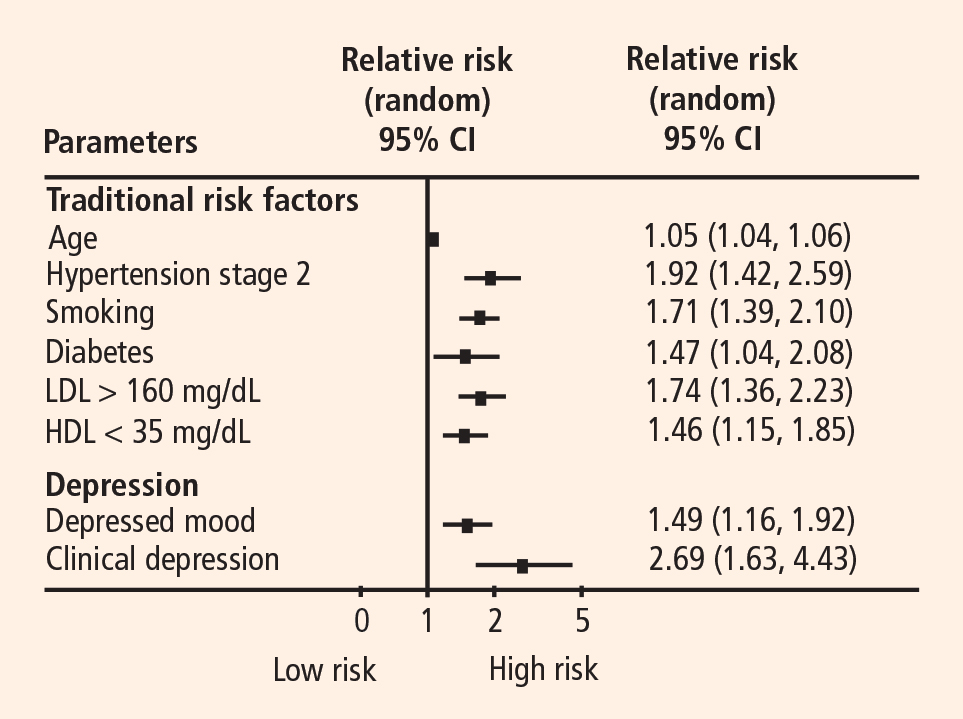
A number of biobehavioral mechanisms have been hypothesized to underlie the relationship between depression and CHD. Most evidence is derived from cross-sectional studies and suggests that depression is associated with traditional risk factors for CHD, such as hypertension, diabetes, and insulin resistance,32,33 as well as changes in platelet reactivity,34 dysregulation of the autonomic nervous system35 and hypothalamic-pituitary-adrenal axis,36 and alterations in the immune response/inflammation.37 Depression is also associated with behavioral factors that are in turn associated with CHD risk, such as reduced treatment adherence,38 smoking,39 and physical inactivity.40