Emotional predictors and behavioral triggers of acute coronary syndrome





ABSTRACT
Mounting evidence suggests that depression, anxiety, and hostility/anger may each be an independent risk factor for acute coronary syndrome (ACS) occurrence. Data specific to the role of these negative emotional states in predisposing to imminent ACS risk are limited, however. Additionally, a number of studies have indicated that certain situational triggers (such as intense physical exertion) and behavioral triggers (such as acute anxiety or anger) are predictive of imminent occurrence of an ACS. Despite these findings, the use of emotional or behavioral information to identify persons at high risk for imminent ACS to facilitate such patient identification.
Anxiety
Anxiety is defined as a future-oriented negative emotion resulting from perceived threat and accompanied by perceived lack of control and lack of predictability.22 Like depression, anxiety occurs along a continuum, but it is characterized as pathological when it becomes chronic, has intensity out of proportion to any real threat, and leaves the affected person with seriously impaired ability to function.
There are many recognized anxiety disorders, including generalized anxiety disorder, panic attacks, obsessive-compulsive disorder, posttraumatic stress syndrome, and various forms of phobia. As a group, these anxiety disorders constitute one of the most common forms of psychiatric illness. Moreover, anxiety disorders and major depression are highly comorbid.23 Although some interesting epidemiologic studies have indicated that anxiety may predict new ACS events,24–26 there are a few that have yielded mixed results.27,28
Hostility and anger
Angry and hostile feelings are overlapping emotions and, when experienced frequently, indicate broader, more enduring temperaments or personality styles. Hostility is a cynical, suspicious, and resentful attitude toward others; negative social exchanges, such as sarcasm or impatience, typify individuals with hostility. In contrast, individuals with anger difficulties can have warm, appropriate interpersonal skills and may display verbal aggression or other outbursts only when provoked. Unlike depressive and anxiety disorders, professionally diagnosed, syndromal anger and hostility are not yet recognized by psychiatric nosology.
Relatively few longitudinal studies have been conducted using measures of hostility in healthy cohorts. These studies have reported both the presence29,30 and the absence31 of positive associations. In a recent systematic review, 7 of 11 studies showed hostility to be a significant risk factor for CHD.8 A case-control study involving participants in the Multiple Risk Factor Intervention Trial (MRFIT) employed a structured interview (as opposed to a questionnaire) designed to elicit information regarding signs of hostility, including irritation, arrogance, uncooperativeness, and angry feelings.30 It revealed that men with high hostility levels were more likely to die of cardiovascular disease than men with low hostility levels (adjusted odds ratio = 1.61; 95% CI, 1.09 to 2.39) in this initially healthy but high-risk cohort.30 The investigators chose the structured interview to overcome participants’ potential to underreport or underrecognize hostile tendencies when completing a questionnaire.30
Over time, specific measurements of chronic anger,32–37 including both unhealthy anger expression34 and suppression,37 have accumulated, permitting examination of their relationship to adverse cardiac outcomes in longitudinal follow-up of disease-free cohorts. A number of these studies have shown a positive association.32,33,35–37 Moreover, a recent report from the Framingham study demonstrated an association between anger/hostility and the development of atrial fibrillation and total-cause mortality over a 10year period,38 and another study has observed a relationship between anger expression and development of stroke.39 Combined, these observations suggest that anger is worthy of further study as a factor in the development of CHD. As with hostility, however, various subscales have been used to study anger, which makes standardization across studies difficult.
Data specific to imminent ACS risk are few
The majority of the negative emotional states have not been tested for their ability to predict an ACS in the near future. Further, negative emotional and cognitive states that may be implicated in the development of CHD or other cardiovascular disease may be quantitatively or even qualitatively different from those psychosocial factors that identify a patient at imminent risk for an ACS.
SITUATIONAL AND BEHAVIORAL TRIGGERS
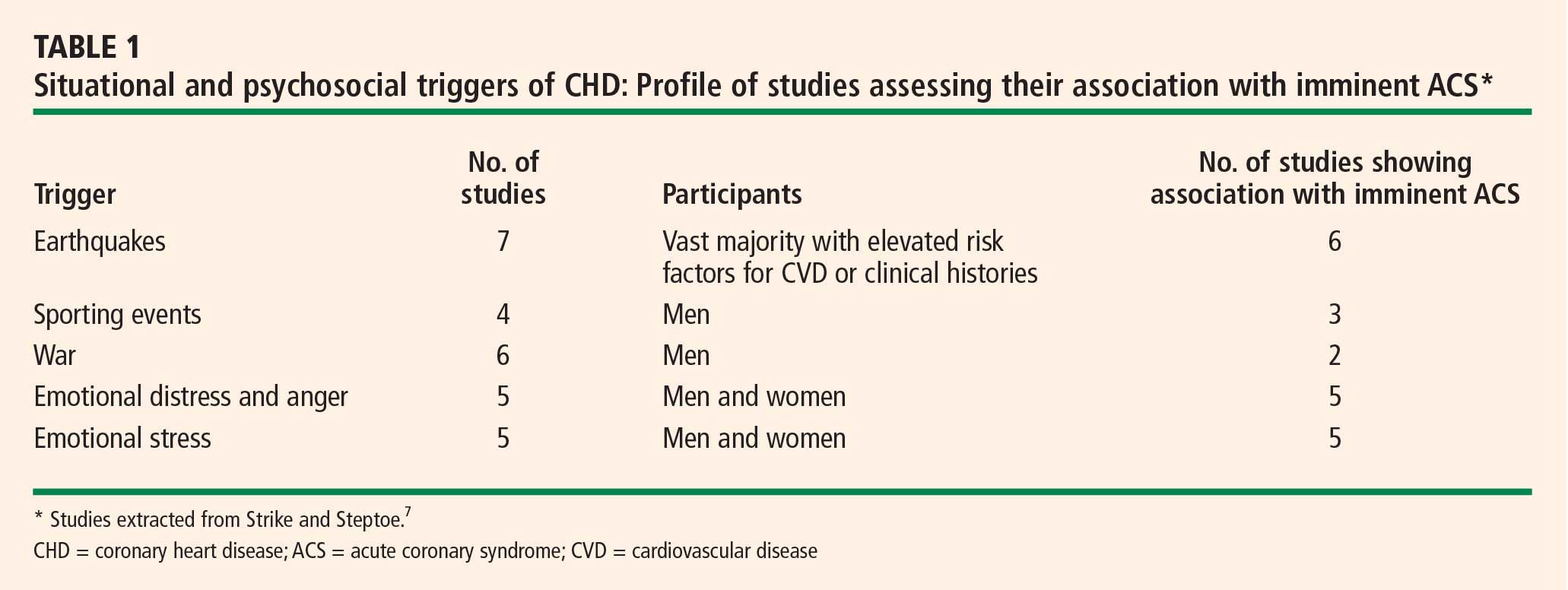
Evidence for imminent risk or trigger status can be obtained from retrospective reports, from witness accounts (if available), or prospectively from electronic diaries coupled with ambulatory electrocardiogram recordings or an implantable cardioverter-defibrillator (ICD). Triggers of an ACS include external stimuli (eg, cocaine use, air pollution, ambient temperature), patient activities (eg, eating a meal high in saturated fat, unusual physical exertion), and emotional reactions such as extreme anger or anxiety.1,2,7,40,41 Myocardial stunning has also been reported immediately after acute emotional stress but has generally been reversible in these cases.42,43 In an observational study, Burg et al found that ICD shocks preceded by an anger episode (as recorded by diary) were more frequent in patients with high trait levels of anger (according to the Speilberger Trait Personality Inventory) and that shocks preceded by an anxiety episode were more frequent in patients with high trait levels of anxiety.44 A systematic review by Strike and Steptoe showed that physical exertion (particularly in poorly conditioned individuals), emotional stress, anger, and extreme excitement are all probable triggers for an ACS.7 A recent meta-analysis suggests that emotional stress immediately precedes MI in approximately 7% of MI cases and is a more frequent ACS trigger for women than for men.1
THE PSYCHOSOCIALLY VULNERABLE PATIENT
This selective overview suggests that patients’ emotional states are frequently implicated in the onset of an ACS but that the use of behavioral or emotional information to identify those at high risk for imminent ACS onset is not yet practical. Triggers are, by definition, state-like, but their impact may be amplified by trait-like characteristics, such as high dispositional anger, anxiety, hostility, or chronic environmental stress.
The previously mentioned analysis of the MRFIT study by Matthews et al30 suggests that patients identified as “high risk” by conventional risk factors, and who additionally possess high trait hostility, should be monitored closely, as they are at risk for cardiovascular death. Additionally, the Burg study of patients with ICDs suggests that arrhythmia may be induced by acute anxiety or anger in those prone to have such emotions chronically.44
Such studies have two research implications. First, controlled laboratory studies that induce acute negative emotion in those with chronic negative emotional states may help reveal the pathophysiologic processes implicated in immediate ACS onset. Interventions for these psychosocially vulnerable patients await such studies. Second, we must begin to consider that in addition to the psychosocially vulnerable patient, we may have psychosocially vulnerable situations, about which we know little at this time.
Acknowledgments
The author thanks Lucia Dettenborn, PhD, for her assistance with the presentation on which this manuscript, in part, is based.
This work was supported by grants HC-25197, HL-76857, HL-80665, and HL84034 from the National Heart, Lung, and Blood Institute. The project described was supported by grant number UL1 RR024156 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH) and the NIH Roadmap for Medical Research, and its contents are solely the responsibility of the author and do not necessarily represent the official view of NCRR or NIH. Information on NCRR is available at https://www.ncrr.nih.gov. Information on Re-engineering the Clinical Research Enterprise can be obtained from https://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp.