Emotional predictors and behavioral triggers of acute coronary syndrome





ABSTRACT
Mounting evidence suggests that depression, anxiety, and hostility/anger may each be an independent risk factor for acute coronary syndrome (ACS) occurrence. Data specific to the role of these negative emotional states in predisposing to imminent ACS risk are limited, however. Additionally, a number of studies have indicated that certain situational triggers (such as intense physical exertion) and behavioral triggers (such as acute anxiety or anger) are predictive of imminent occurrence of an ACS. Despite these findings, the use of emotional or behavioral information to identify persons at high risk for imminent ACS to facilitate such patient identification.
Numerous systematic reviews indicate that psychosocial factors are predictive of an initial acute coronary syndrome (ACS),1–8 defined as myocardial infarction (MI), unstable angina, or sudden cardiac death. Psychosocial factors under active investigation for their role in ACS onset include chronic negative emotional states (eg, depression, hostility, anxiety) as well as situational and behavioral triggers (eg, acute anger, unusual intense physical activity). This review will present evidence for each grouping of risk markers and then discuss the studies required to better identify and treat patients who have these psychosocial vulnerabilities.
NEGATIVE EMOTIONAL STATES
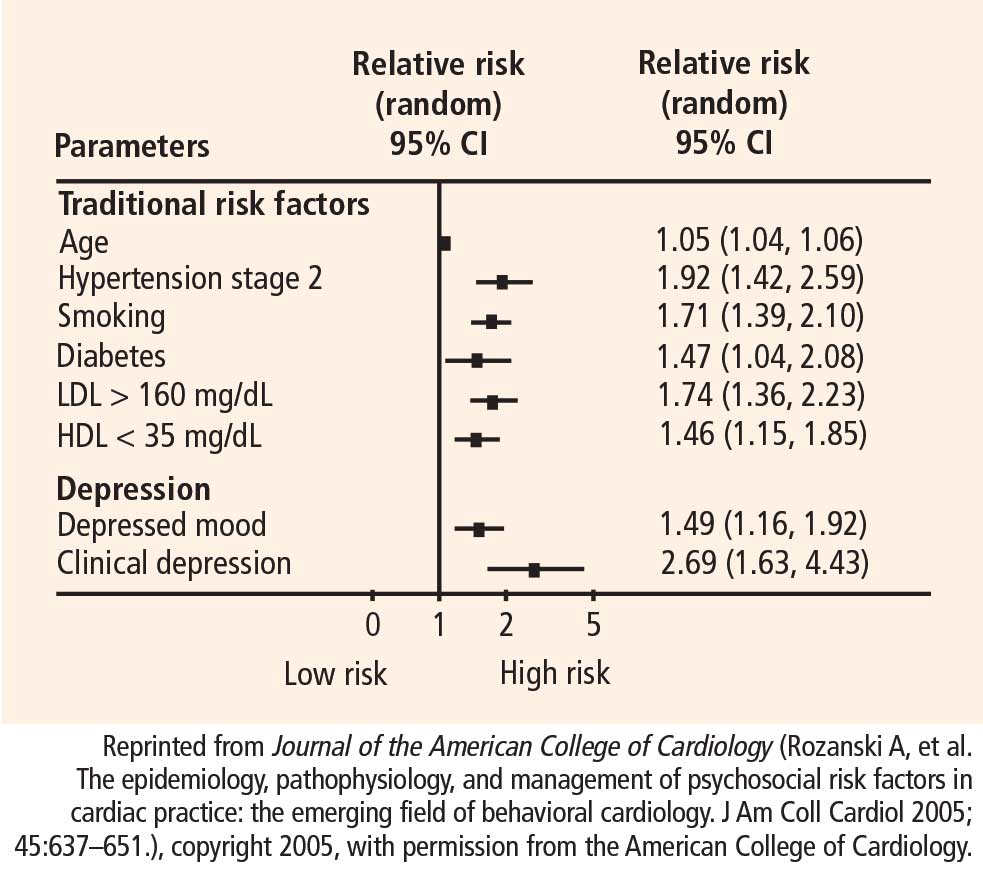
Increasing epidemiologic and pathophysiologic evidence suggests that depression, anxiety, and hostility/anger may each be an independent risk factor for initial occurrence of a cardiovascular event.4,8 The vast majority of evidence has been accumulated for depression, and many meta-analyses and systematic reviews now indicate that depression—as either a clinical diagnosis or an elevation in self-reported symptoms—is a strong, consistent, independent predictor of ACS incidence.9–11
Major depression
Major depressive disorder is most appropriately diagnosed through direct patient interview, preferably by trained professionals who look for evidence of severely depressed mood lasting at least 2 consecutive weeks, other concomitant symptoms (such as change in eating or sleeping habits), and evidence of associated functional impairment. Because this interview approach is not convenient for large epidemiologic studies, evaluation of major depression by interview in longitudinal epidemiologic studies has been sparse,12,13 and only a limited number of other studies have also evaluated the role of a history of depressive disorders14 or a history of depression treatment.14–18
Depressive symptoms
The impact of self-reported depressive symptoms on cardiac outcomes has been studied more widely.in community settings, among the elderly, and in various cardiac settings.using scales such as the Beck Depression Inventory and the Center for Epidemiological Studies Depression Scale. Notably, these scales assess only the presence of recent depressive symptoms. Nevertheless, despite this important limitation, one-time assessment of healthy participants using these scales has generally revealed a significant relationship between depressive symptoms and future adverse cardiac events.9,18 As further evidence of a gradient relationship, the frequency of cardiac events increases as the level of depressive symptoms increases.13,19
Depression is a complex phenotype, and some have argued that subtypes, or intermediary phenotypes, of depression may be particularly predictive of ACS incidence and recurrence.20 Interestingly, the first article ever published documenting a link between depression and coronary artery disease focused exclusively on melancholic depression, or endogenous depression.21