Postoperative pulmonary complications: An update on risk assessment and reduction





ABSTRACT
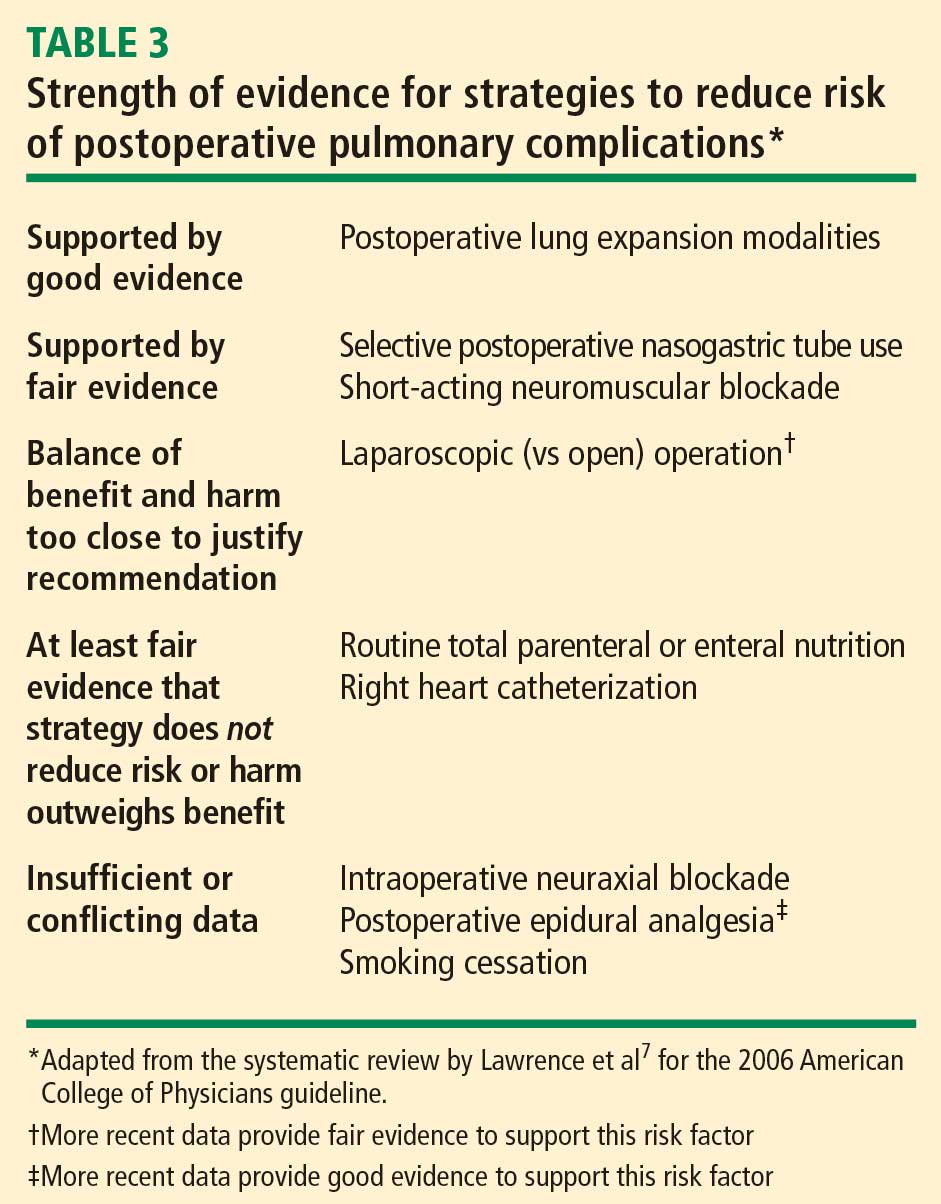
Postoperative pulmonary complications are common, serious, and expensive. Important predictors of risk are advanced age, poor health as assessed by American Society of Anesthesiologists class, and surgery near the diaphragm. Effective strategies to reduce risk include postoperative lung expansion techniques, preoperative intensive inspiratory muscle training, postoperative thoracic epidural analgesia, selective rather than routine use of nasogastric tubes, and laparoscopic rather than open bariatric surgery.
KEY POINTS
- Pulmonary complications are as common as cardiac complications following noncardiac surgery.
- Surgical site is the most important predictor of risk for postoperative pulmonary complications: aortic, thoracic, and upper abdominal surgeries are high-risk procedures, even in healthy patients.
- Obstructive sleep apnea and pulmonary hypertension have recently been identified as risk factors, but the limited available evidence does not support preoperative screening for these conditions in patients without symptoms.
- Postoperative continuous positive airway pressure therapy is effective for reducing pulmonary complications in patients who are unable to perform deep breathing or incentive spirometry exercises.
- The jury is out on whether smoking cessation shortly before surgery lowers risk for postoperative pulmonary complications.
STRATEGIES FOR RISK REDUCTION
Postoperative CPAP: Good option when exercise ability is limited
Among the postoperative lung expansion modalities, continuous positive airway pressure (CPAP) is particularly useful for patients who are unable to perform deep breathing or incentive spirometry exercises. A recent systematic literature review identified nine randomized controlled trials of CPAP vs standard therapy in a total of 654 patients undergoing abdominal surgery.13 Meta-analysis of these studies showed that CPAP was associated with significant reductions in the risk of overall postoperative pulmonary complications (odds ratio [OR] = 0.66; 95% CI, 0.52–0.85), atelectasis (OR = 0.75; 95% CI, 0.58–0.97), and pneumonia (OR = 0.33; 95% CI, 0.14–0.75) relative to standard therapy.
Use nasogastric tubes selectively
Nasogastric tubes can be used either routinely following abdominal surgery or only in select patients—eg, those who have symptomatic abdominal distention or nausea. The difference is important since nasogastric tubes may potentially increase the risk of aspiration and thus lead to a pulmonary complication. Nelson et al conducted a meta-analysis of 24 studies that compared routine nasogastric tube use in abdominal surgery with selective use based on symptoms or abdominal distention.14 They found that routine use was associated with a significant increase in postoperative pulmonary complications (OR = 1.45; 95% CI, 1.08–1.93) relative to selective use, without achieving any of its intended goals.
Laparoscopic vs open surgery: Evidence begins to follow intuition
Intuitively, it seems that laparoscopic procedures should reduce risk for postoperative pulmonary complications compared with open surgical procedures, as they are associated with less postoperative pain, which should facilitate deep breathing and improve postoperative lung volumes. Nevertheless, evidence for whether laparoscopic surgery reduces the risk of pulmonary complications has been mixed until recently.
In 2008, however, Weller and Rosati published an analysis of a nationally representative database of 19,156 patients who underwent bariatric surgery in 2005.15 After adjusting for comorbidities, they found that the rate of postoperative pulmonary complications was nearly double if patients underwent open surgery as opposed to laparoscopic surgery (OR = 1.92; 95% CI, 1.54–2.38). Open surgery was also associated with significantly higher rates of sepsis, cardiovascular events, and reoperation compared with laparoscopic procedures. This study suggests that choosing laparoscopic procedures is another strategy that may reduce pulmonary complication rates, at least in the setting of bariatric surgery.
Postoperative thoracic epidural analgesia
Question: Thoracic epidural analgesia reduces rates of which of the following?
A. Pneumonia following abdominal aortic aneurysm repair
B. Pulmonary complications following coronary bypass surgery
C. Respiratory failure following abdominal surgery
D. All of the above
The correct answer is D. Thoracic epidural analgesia is another important strategy for reducing postoperative pulmonary complications, as demonstrated by a 2007 systematic literature review by Liu and Wu.16 Their analysis showed that rates of pneumonia, respiratory failure, and pulmonary complications overall were reduced by approximately one-third to more than one-half with the use of postoperative thoracic epidural analgesia in patients undergoing aortic aneurysm repair, coronary bypass surgery, and abdominal surgery.
Smoking cessation: The jury is still out
Whether preoperative cigarette cessation reduces pulmonary complication rates has been controversial over the past decade. Early reports showed that among patients who smoke, those who quit shortly before surgery actually had higher complication rates than patients who continued to smoke. The most reasonable explanation seems to be that many patients who stop smoking report increased coughing and sputum production for the first month or two. Selection bias also may have played a role in these findings.
More recently, two randomized trials studied the impact of perioperative smoking intervention programs involving counseling and nicotine replacement.17,18 Unfortunately, both studies primarily studied patients undergoing low-risk procedures and were insufficiently powered to show a difference in pulmonary complication rates. The question of whether smoking cessation is an effective strategy to reduce postoperative pulmonary risk remains unanswered.
Preoperative intensive lung expansion: A promising new intervention
While the effectiveness of postoperative lung expansion techniques is undisputed,7 preoperative lung expansion—also known as inspiratory muscle training—has only recently been investigated. Hulzebos et al randomized 279 patients undergoing coronary artery bypass graft surgery who were at high risk for developing pulmonary complications to either usual care or inspiratory muscle training.19 The latter intervention involved 20 minutes per day of incentive spirometry, active breathing, and forced expiration techniques for at least 2 weeks prior to surgery. Rates of high-grade postoperative pulmonary complications were cut in half (OR = 0.52; 95% CI, 0.30–0.92) and rates of pneumonia were reduced by 60% (OR = 0.40; 95% CI, 0.19–0.84) in patients who received inspiratory muscle training relative to the usual-care group.
In clinical practice, preoperative inspiratory muscle training can be done in a chest physical therapy outpatient setting or a pulmonary rehabilitation clinic in the hospital.