Postoperative pulmonary complications: An update on risk assessment and reduction





ABSTRACT
Postoperative pulmonary complications are common, serious, and expensive. Important predictors of risk are advanced age, poor health as assessed by American Society of Anesthesiologists class, and surgery near the diaphragm. Effective strategies to reduce risk include postoperative lung expansion techniques, preoperative intensive inspiratory muscle training, postoperative thoracic epidural analgesia, selective rather than routine use of nasogastric tubes, and laparoscopic rather than open bariatric surgery.
KEY POINTS
- Pulmonary complications are as common as cardiac complications following noncardiac surgery.
- Surgical site is the most important predictor of risk for postoperative pulmonary complications: aortic, thoracic, and upper abdominal surgeries are high-risk procedures, even in healthy patients.
- Obstructive sleep apnea and pulmonary hypertension have recently been identified as risk factors, but the limited available evidence does not support preoperative screening for these conditions in patients without symptoms.
- Postoperative continuous positive airway pressure therapy is effective for reducing pulmonary complications in patients who are unable to perform deep breathing or incentive spirometry exercises.
- The jury is out on whether smoking cessation shortly before surgery lowers risk for postoperative pulmonary complications.
Newly identified risk factors
Question: Which of the following has recently been identified as a risk factor for postoperative pulmonary complications?
A. Epidural anesthesia
B. Insulin-treated diabetes
C. Obstructive sleep apnea
D. Immobility
The correct answer is C. There is no evidence that epidural anesthesia or insulin-treated diabetes are risk factors. Immobility seems intuitively correct but has not emerged as a risk factor among high-quality studies in the literature.
Obstructive sleep apnea. The role of obstructive sleep apnea was unclear prior to publication of new data in the last couple of years. Hwang et al enrolled 172 patients who were soon to have elective surgery and had at least two of four clinical features of obstructive sleep apnea (snoring, daytime somnolence, witnessed apnea event, or crowded oropharynx).8 Patients underwent nocturnal oximetry before surgery and were divided into two groups based on number of desaturation episodes per hour. Patients with five or more desaturations had markedly higher rates of postoperative respiratory complications (8 complications among 98 patients) than did patients with fewer than five desaturations (1 complication among 74 patients). The presence of five or more desaturations was also associated with higher rates of cardiac, gastrointestinal, and bleeding complications. Though this was a small study, its results suggest a significant association between obstructive sleep apnea and pulmonary complications.
The issue of whether to screen patients for obstructive sleep apnea before major noncardiac surgery is still unresolved.
Pulmonary hypertension has also been identified as a risk factor in recent years with the publication of two studies that estimated its impact on morbidity and mortality after major noncardiac surgery.9,10 One of the studies, a retrospective database review, found a 28% incidence of respiratory failure among 145 surgical patients with pulmonary hypertension.9 In the other study, a prospective case-control trial, respiratory failure occurred in 21% of patients with pulmonary hypertension compared with only 3% of matched controls.10 In the case-control study, pulmonary hypertension was also associated with significantly elevated rates of heart failure and in-hospital death.
The results of these studies do not support preoperative screening for undiagnosed pulmonary hypertension, but they do underscore the need to recognize established pulmonary hypertension as an important risk factor for postoperative complications.
AN UPDATED INDEX FOR RESPIRATORY FAILURE
Several years ago, investigators from the Veterans Affairs Medical Centers developed a respiratory failure index using a design similar to those of well-established indices for cardiac risk.11 The same group also developed a separate risk index for pneumonia.12
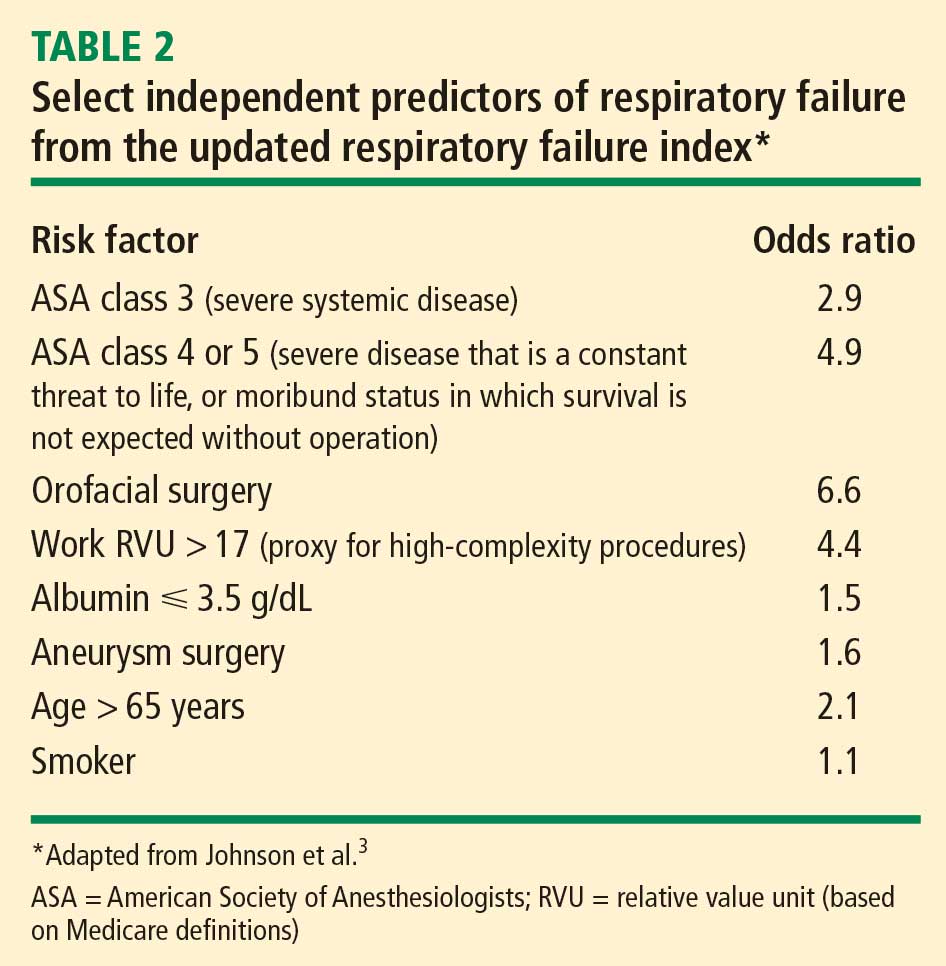
This respiratory failure index was recently updated3 to reflect experience from private and academic hospitals, making the results more generally applicable. The researchers evaluated data from 180,000 patients undergoing major general or vascular surgery (defined according to the NSQIP) over a 3-year period. Respiratory failure was defined as requiring at least 48 hours of ventilation or unplanned reintubation.
Comparison and contrast with the ACP guideline
Question: How does the updated respiratory failure index differ most significantly from the 2006 ACP guideline?
A. New index places greater emphasis on ASA class
B. New index offers a simplified weighted point scheme
C. New index ranks low albumin as a less important risk factor
D. New index attributes low risk to cigarette use
The correct answer is C: low albumin is a minor risk factor in the respiratory failure index, whereas it was one of the single most important predictors in the ACP guideline. As for the other answer choices, the new index places about the same emphasis on ASA class and cigarette use as does the ACP guideline, and it does not offer a simplified approach, as it incorporates 28 different factors.
Overall, most risk factors were similar in the updated respiratory failure index and the ACP guideline, but the index differs in several important ways:
- The index assigns less risk to low albumin, functional dependence, and congestive heart failure
- The index assigns greater risk to orofacial surgery
- The index identifies several new risk factors—high-complexity surgery, preoperative sepsis, ascites, and hypernatremia (serum sodium > 145 mmol/L).