Perioperative management of diabetes: Translating evidence into practice





ABSTRACT
Glycemic control before, during, and after surgery reduces the risk of infectious complications; in critically ill surgical patients, intensive glycemic control may reduce mortality as well. The preoperative assessment is important in determining risk status and determining optimal management to avoid clinically significant hyper- or hypoglycemia. While patients with type 1 diabetes should receive insulin replacement at all times, regardless of nutritional status, those with type 2 diabetes may need to stop oral medications prior to surgery and might require insulin therapy to maintain blood glucose control. The glycemic target in the perioperative period needs to be clearly communicated so that proper insulin replacement, consisting of basal (long-acting), prandial (rapid-acting), and supplemental (rapid-acting) insulin can be implemented for optimal glycemic control. The postoperative transition to subcutaneous insulin, if needed, can begin 12 to 24 hours before discontinuing intravenous insulin, by reinitiation of basal insulin replacement. Basal/bolus insulin regimens are safer and more effective in hospitalized patients than supplemental-scale regular insulin.
KEY POINTS
- Surgery and anesthesia can induce hormonal and inflammatory stressors that increase the risk of complications in patients with diabetes.
- Elevated blood glucose levels are associated with worse outcomes in surgical patients, even among those not diagnosed with diabetes.
- The perioperative glycemic target in critically ill patients is 140 to 180 mg/dL. Evidence for a target in patients who are not critically ill is less robust, though fasting levels less than 140 mg/dL and random levels less than 180 mg/dL are appropriate.
- Postoperative nutrition-related insulin needs vary by nutrition type (parenteral or enteral), but ideally all regimens should incorporate a basal/bolus approach to insulin replacement.
ELEMENTS OF PHYSIOLOGIC INSULIN REPLACEMENT
In hospitalized patients with hyperglycemia, three different components of insulin replacement require management1:
Basal insulin replacement consists of a long-acting insulin preparation administered regardless of the patient’s oral intake status, with the premise of matching hepatic (endogenous) glucose production
Prandial insulin replacement requires a rapid-acting insulin preparation given to cover nutritional needs
Supplemental (or correction) insulin replacement requires a rapid-acting preparation (usually the same insulin type as for prandial coverage) to correct blood glucose values that exceed predetermined glycemic targets.
For most patients, basal insulin replacement might be appropriate preoperatively to control fasting glucose, whereas during surgery, especially if prolonged or high risk, an intravenous (IV) insulin drip is the most effective means of glucose control. The postoperative transition from the IV insulin drip usually involves basal insulin replacement plus supplemental rapid-acting insulin. Prandial or nutritional insulin should be started once the patient begins to receive nutrition (oral, enteral, or hyperalimentation).
GOALS OF PERIOPERATIVE GLYCEMIC CONTROL
Perioperative glycemic management has several key objectives:
- Avoidance of clinically significant hyper- or hypoglycemia
- Maintenance of electrolyte and fluid balance
- Prevention of ketoacidosis, which is imperative in patients with type 1 diabetes, who require insulin at all times
- Achievement of specific glycemic targets, as discussed above—ie, less than 180 mg/dL in critically ill patients and less than 140 mg/dL in stable patients.13
Strategies differ across the perioperative timeline
Strategies for perioperative glycemic control differ before, during, and after surgery, as summarized immediately below and detailed in the following sections.
Preoperatively, glycemia should be stabilized, typically with subcutaneous insulin, if there is enough time to do so. For patients who have not previously been on insulin, placing them on an insulin supplemental scale to correct glycemia to desired targets might be a first step. In the setting of hyperglycemia, these patients may also be started on a low dose of basal insulin, with preference given to basal insulin analogs, given their consistent and relatively peakless action profile and lower risk of hypoglycemia. A starting dose of 0.2 to 0.4 U/kg is appropriate and carries a low risk of hypoglycemia. For patients already using insulin on an outpatient basis, continuing their basal insulin dose, possibly at a reduced dosage (25% less), together with supplemental-scale insulin coverage, should stabilize blood glucose levels. For patients on combination insulin or premixed insulin types, the basal insulin dose for preoperative management can be estimated by taking the patient’s usual total daily dose and delivering 40% to 50% of that dose as a basal insulin analog injection. Clearly, a supplemental scale should be implemented along with basal insulin replacement.
Intraoperatively, switching to IV insulin may be appropriate for stabilizing glycemia, depending on the type of surgery. A number of IV insulin protocols have been proposed, although no consistent comparisons of efficacy or safety among these protocols have been published.
Postoperatively, patients eventually should be transitioned from IV to subcutaneous insulin when glycemic control stabilizes. This transition may be complicated for many reasons. Oral intake may be inconsistent. The surgery and surrounding environment can induce stressors, promote susceptibility to infection, and increase insulin resistance. Additionally, some patients may be on hyperalimentation. Specific instructions for the transition from IV to subcutaneous insulin are covered later in this article.
PREOPERATIVE GLYCEMIC MANAGEMENT
In patients with type 2 diabetes, oral agents pose certain safety risks and should be discontinued prior to surgery.
Sulfonylureas may induce hypoglycemia in patients who are placed on NPO (“nothing by mouth”) orders and should be held in patients who are fasting.
Metformin can induce lactic acidosis if kidney function declines and should be withheld 1 to 2 days before planned surgery if a need for IV contrast is anticipated or the procedure could potentially lead to hemodynamic instability and reduced renal perfusion.
Thiazolidinediones may cause fluid retention that can complicate the postoperative period; they can be discontinued several days prior to a planned surgery.
GLP-1 agonists, such as exenatide, can slow gastric motility and potentially delay gastrointestinal recovery after major surgery; they should be held the day of surgery.
DPP-4 inhibitors (incretin enhancers), such as sitagliptin, do not have significant side effects and, if need be, can be continued. Because incretin therapies act via a glucose-dependent mechanism, they are unlikely to cause hypoglycemia, even in a patient whose oral intake is held or delayed. On the other hand, since their effect is mostly in reducing postprandial glycemia, there may be little need to use them in a patient who is NPO.
Patients with type 1 diabetes must continue basal insulin replacement preoperatively (0.2 to 0.3 U/kg/day of a long-acting insulin). Patients with type 2 diabetes may benefit from basal insulin replacement, as previously noted.
Supplemental insulin scales are used to correct hyperglycemia regardless of a patient’s oral intake status. They can be individualized based on the estimated total daily insulin dose and require glycemic targets to be established. Fingerstick glucose monitoring should be done every 4 to 6 hours in a patient who is NPO, and supplemental-scale insulin should be used to correct glucose values that exceed target. For supplemental-scale coverage, rapid-acting insulin analogs have a shorter duration of action than human regular insulin and may be given subcutaneously every 4 to 6 hours, whereas regular insulin should not be given more often than every 6 hours to correct hyperglycemia. These differences in action duration should be kept in mind to minimize the potential for insulin stacking.
INTRAOPERATIVE GLYCEMIC MANAGEMENT
Procedure length is an important determinant
Strategies for intraoperative glucose management vary according to the length of the procedure.
For minor, short procedures, the preoperative glucose management orders may be continued.
For longer, more complex procedures, a switch to an IV insulin drip is safe and allows rapid adjustments in dosing and plasma glucose levels. Ideally, IV insulin is started prior to the procedure so that the glucose level is stable once the patient arrives in the operating room. Given the logistics of IV insulin management, including the need for frequent monitoring (hourly) and dose adjustments, this type of treatment should be reserved for environments with adequate numbers of trained staff.
IV regular insulin is therapy of choice
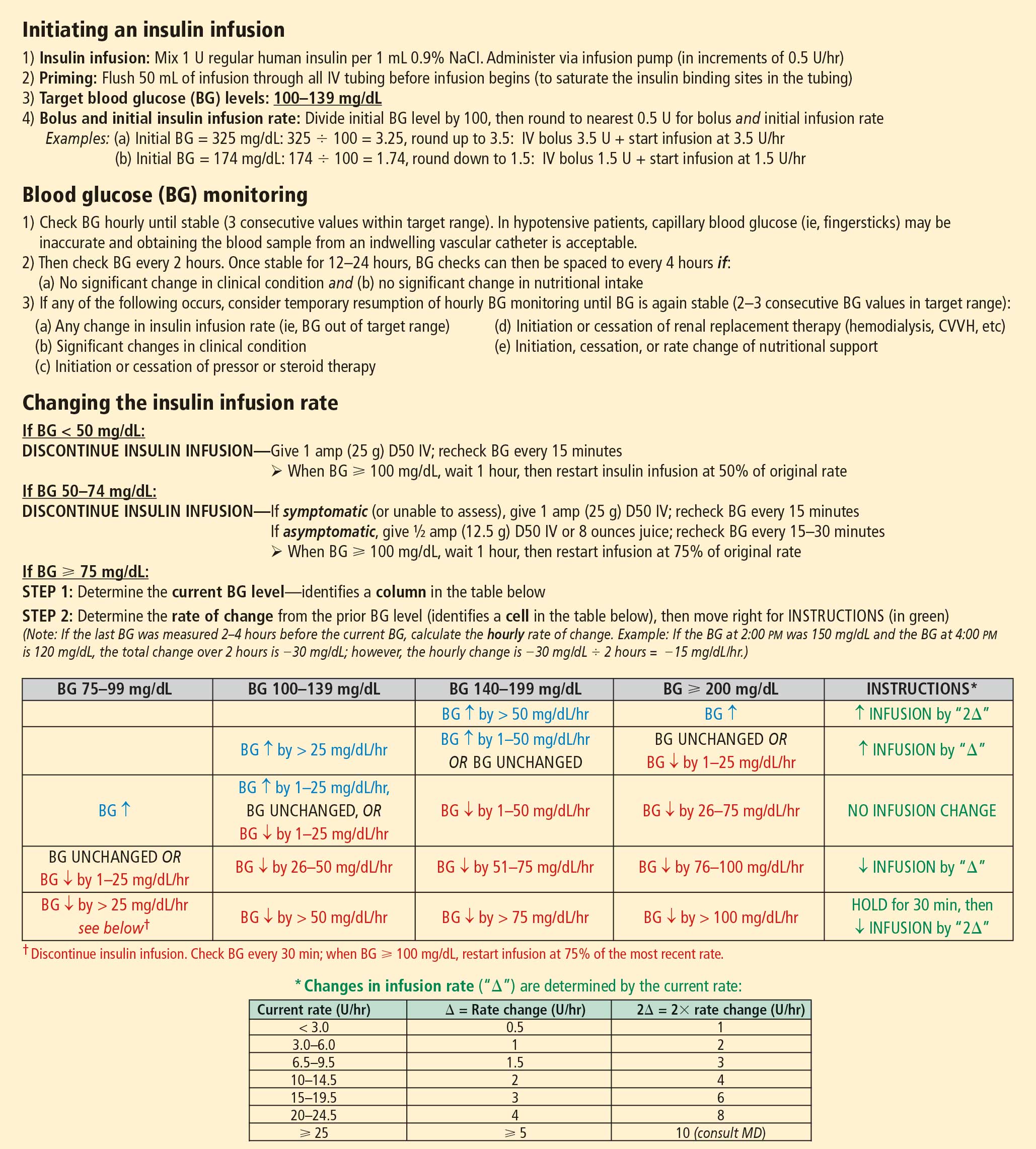
Several different algorithms for IV regular insulin therapy are in use. Some are static, such as those of Markovitz et al14 and Stockton et al,15 while others are dynamic (ie, doses are self-adjusted based on changes in blood glucose level), such as the “Yale protocol” of Goldberg et al (Figure 1).16