Psychiatric Morbidity in Patients With Psoriasis





Psoriasis is a common skin disorder that is associated with impairments in quality of life (QOL) and psychological distress. In this study, we investigated the prevalence and determinants of psychiatric morbidity (ie, psychiatric disorders) in 104 patients with chronic plaque psoriasis who presented to the Departments of Dermatology, Venereology, and Leprology at a tertiary-level teaching hospital in North India. A 2-stage, cross-sectional study using standardized self-assessment questionnaires assessing psoriasis severity and QOL were administered followed by an evaluation conducted by a psychiatrist. Our findings suggest a need for effective screening for psychiatric disorders in psoriasis patients, greater sensitivity among dermatologists to the association of impairments in QOL and psychiatric morbidity with this condition, and collaboration with mental health professionals to ensure better treatment outcomes in psoriasis patients.
Practice Points
- Psychiatric disorders, especially depressive disorders, are common in patients with psoriasis.
- Impairments in quality of life in patients with psoriasis can predict psychiatric morbidity.
- Screening for psychiatric disorders and depression in particular should be considered in patients with psoriasis.
- Treatment should focus not just on symptom alleviation but also coping with the effects of living with a chronic illness such as psoriasis and improving quality of life.
Results
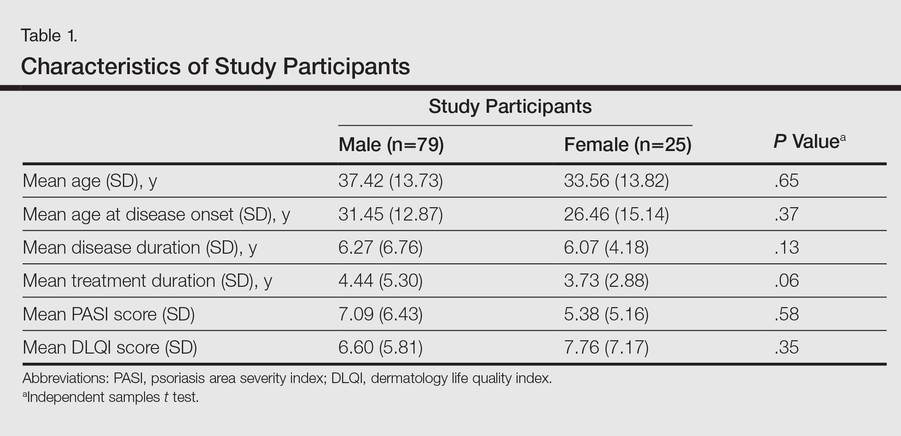
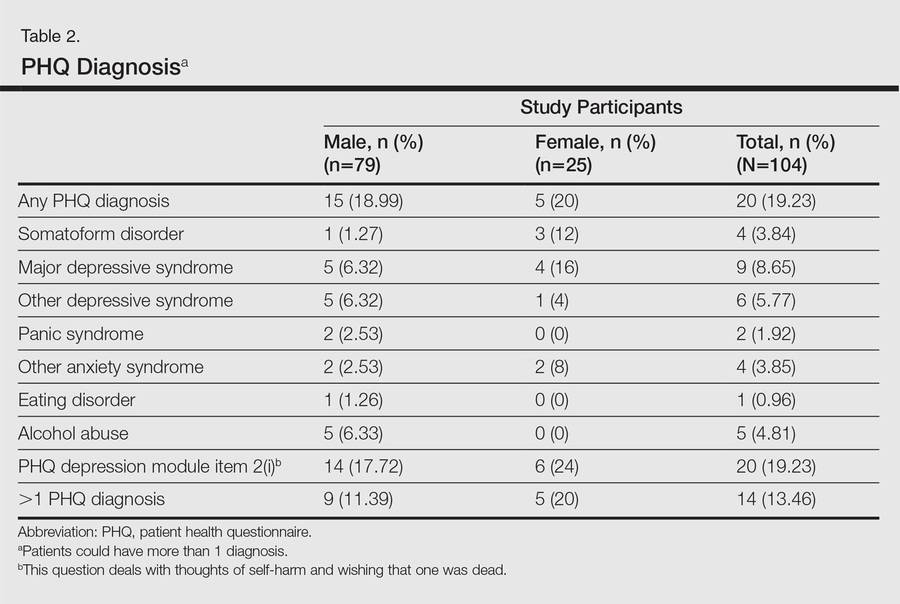
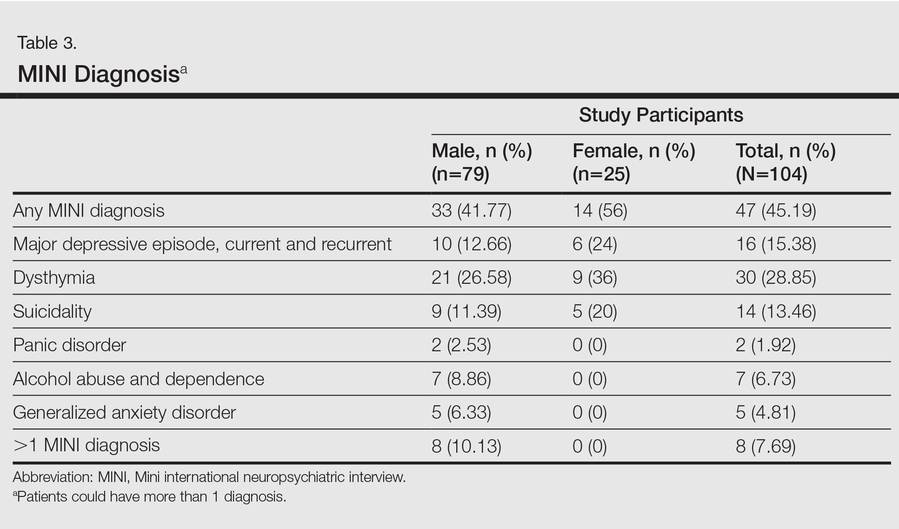
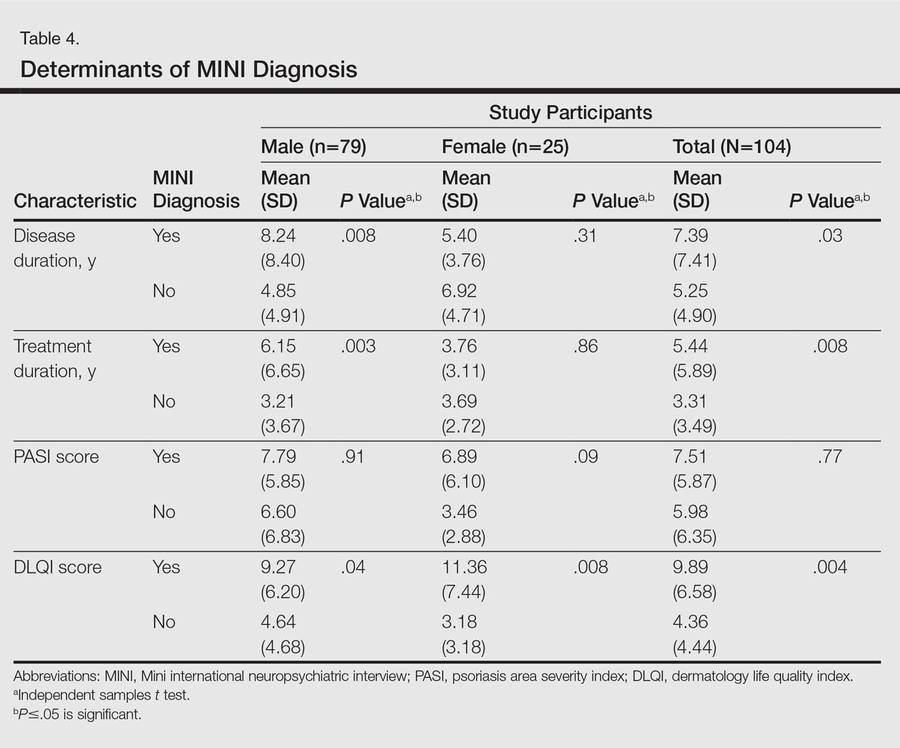
One hundred four participants were included in this study. The sociodemographic, clinical, and diagnostic profiles, as well as the determinants of MINI diagnosis, are provided in Tables 1 through 4. The PASI and DLQI scores indicated that most participants had mild to moderate psoriasis severity.10 The prevalence of alcohol-related disorders was only found in the male subpopulation, which is consistent with the sociocultural context of North India. Psoriasis severity (ie, PASI score) was not found to be a determinant of psychiatric diagnoses in the study population. There was no statistical difference in measures of current clinical status and treatment modality when those with or without any psychiatric diagnoses were compared. When the variables of disease duration, treatment duration, and DLQI were entered into a binary logistic regression with positive status for a MINI diagnosis as a dependent variable indicating the presence of a psychiatric disorder, it was found that the DLQI score was a significant predictor (b=0.19; SE=0.47; χ2=17.92; P<.05). This finding was the same for regression analyses for males and females separately and also for DD as a dependent variable.
Mean DLQI and PASI scores were positively correlated with each other (Pearson r=0.23; P=.01). This relationship was maintained in males (Pearson r=0.24; P=.03) but not in females (Pearson r=0.14; P=.30). The correlations between DLQI and PASI scores and both disease duration and treatment duration were not significant. The Cohen κ values for the interrater reliability analyses done to assess the concordance of the PHQ and MINI diagnostic groups were modest (0.31-0.42), which was true even when MINI depressive disorders without dysthymia and PHQ depressive disorders were compared.