Minding menopause: Psychotropics vs. estrogen? What you need to know now






Psychotropics have become a first-line therapy for hot flashes and depression in perimenopause. Will you be ready when Ob/Gyns call you for help?
Oral estrogen replacement therapy reduces bioavailable testosterone by 42% on average, which can induce androgen deficiency in a menopausal woman.19 The increased estrogen inhibits pituitary LH and decreases stimulation of the androgen-producing cells in the ovary.20
Female androgen deficiency. A number of papers have been published on female androgen deficiency syndrome (FADS).21 Its diagnosis requires symptoms of thinning pubic and axillary hair, decreased body odor, lethargy, low mood, diminished well-being, and declining libido and orgasm, despite adequate estrogen but low levels of testosterone and DHEA.
TREATING TESTOSTERONE DEFICIENCY
Benefits of replacement therapy. Replacing testosterone in women with FADS can improve mood, well-being, motivation, cognition, sexual function related to libido, orgasm, sexual fantasies, desire to masturbate, and nipple and clitoral sensitivity.22 Muscle and bone stimulation and decreased hot flashes are also reported.23 Women with androgen deficiency symptoms and low testosterone at menopause should at least be considered for physiologic testosterone replacement.
Risks of replacement therapy. Androgen replacement therapy does carry some risks, which need to be discussed with the patient. Testosterone may lower levels of beneficial HDL cholesterol, so get the cardiologist’s clearance before you give testosterone to a woman with heart disease or an HDL cholesterol level <45 mg/dL.
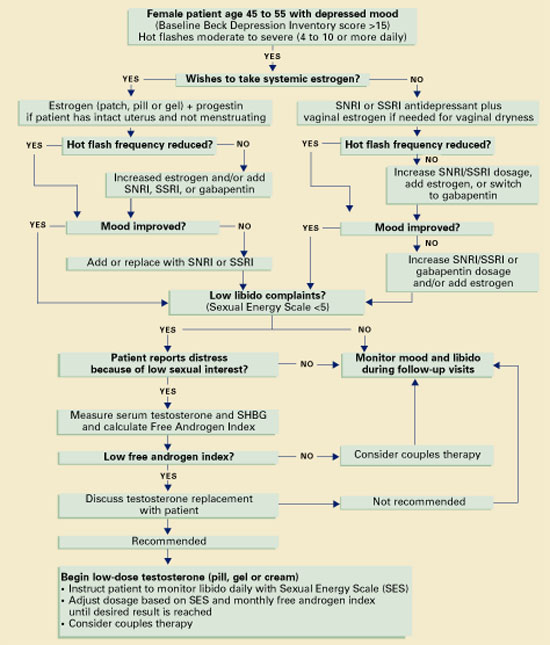
Algorithm Managing mood and libido problems during perimenopause
A meta-analysis of eight clinical trials found no changes in liver function in menopausal women taking 1.25 to 2.5 mg/d of methyl testosterone. Liver toxicity has been reported in men using 10-fold higher testosterone dosages.24
At the normal level of testosterone, darkening and thickening of facial hair are rare in light-skinned, light-haired women but can occur in dark-skinned, dark-haired women. Increased irritability, excess energy, argumentativeness, and aggressive behavior have been noted if testosterone levels exceed the physiologic range.
Controlled, randomized studies are needed to assess the effects of long-term use (more than 24 months) of testosterone replacement in women.
Challenges in measuring testosterone levels. Serum free testosterone is the most reliable indicator of a woman’s androgen status, but accurately measuring testosterone levels is tricky:
- Only 2% of circulating testosterone is unbound and biologically active; the rest is bound to sex hormone-binding globulin (SHBG) or albumin.
- In ovulating women, serum testosterone levels are higher in the morning than later in the day and vary greatly within the menstrual cycle.
- Levels of androgens and estrogen are highest during the middle one-third of the cycle—on days 10 to 16, counting the first day of menstrual bleeding as day 1.25
- Oral contraceptives also decrease androgen production by the ovary and can result in low libido in some women.26
Tests developed to measure testosterone levels in men are not sensitive enough to accurately measure women’s naturally lower serum concentrations, let alone the even lower levels characteristic of female androgen or testosterone deficiency. New measurements and standardization of normal reference ranges have been developed for women complaining of low libido.27
Tests for androgen deficiency include total testosterone, free testosterone, DHEA, and DHEAS. Measuring SHBG will help you determine the free, biologically active testosterone level and calculate the Free Androgen Index (FAI) for women (Table 3).28
Table 3
Free androgen index (FAI) values in women, by age
| Replacing a woman’s bioactive testosterone to the normal free androgen index range for her age may improve low libido. | |
| How to calculate FAI | |
| Total testosterone in nmol/L (total testosterone in ng/ml X 0.0347 X 100), divided by sex hormone-binding globulin (SHBG) in nmol/L. | |
| Age | Normal range |
| 20 to 29 | 3.72 to 4.96 |
| 30 to 39 | 2.04 to 2.96 |
| 40 to 49 | 1.98 to 2.94 |
| 50 to 59+ | 1.78 to 2.86 |
| Source: Guay et al, reference 28. | |
A candidate for testosterone therapy?
Now that Anne’s mood, sleep, and hot flashes have improved with venlafaxine, she wants help with her lack of sexual interest. You measure her testosterone and SHBG levels and find that her free androgen index is very low at 0.51 (normal range, 1.78 to 2.86).
In collaboration with her Ob/Gyn, you and Anne decide to start her on testosterone replacement therapy. You prescribe Androgel, starting at 1/7th of a 2.5-mg foil packet (0.35 mg/d of testosterone), and instruct her to rate her sexual energy daily, using a Sexual Energy Scale.
TESTOSTERONE CHOICES FOR WOMEN
Replacing a woman’s bioactive testosterone level to the normal free androgen index range for her age group may improve low libido. Some low-dose testosterone replacement options include:
- methyl testosterone sublingual pills, 0.5 mg/d, made by a compounding pharmacy or reduced dosages of oral pills made for men. If you prescribe methyl testosterone, routine lab tests will not accurately measure serum testosterone levels—unless you order the very expensive test that is specific for methyl testosterone.
- 2% vaginal cream, applied topically to increase clitoral and genital sensitivity. It may increase blood levels moderately through absorption
- Androgel, a topical testosterone approved for men. As in Anne’s case, start with 0.35 mg/d or one-seventh of the 2.5 mg packet (ask the pharmacist to place this amount in a syringe). Instruct the patient to apply the gel to hairless skin, such as inside the forearm. Effects last about 24 hours, and you can measure serum levels accurately after 14 days. Vaginal throbbing—a normal response—may occur within 30 minutes of testosterone application.