Consider retroperitoneal packing for postpartum hemorrhage






For intractable bleeding, this technique, borrowed from pelvic trauma surgery, allows you to stabilize the patient until her underlying injury can be addressed
IN THIS ARTICLE
Four laparotomy sponges are packed along the retroperitoneal space to provide tamponade (FIGURE 3). Within seconds, the patient stabilizes, with systolic blood pressure rising to 90 mm Hg and the heart rate declining toward 100 bpm. Bleeding ceases immediately, and the hysterectomy is completed under stable conditions without further blood loss.

FIGURE 1 Packing begins with a 5-cm incision
Make a 5-cm incision just cephalad to the symphysis pubis, deep to the fascia, and into the space of Retzius.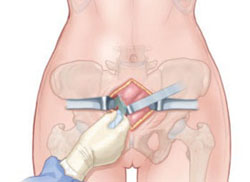
FIGURE 2 Preparing to place sponges
Use blunt dissection in the space of Retzius before placing packing material.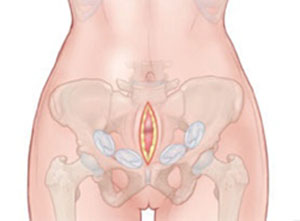
FIGURE 3 Insert packing into retroperitoneal space
Packing is usually sufficient when two or three laparotomy sponges are placed at each side of the retroperitoneal pelvis.
How retroperitoneal packing saves lives
Most of the pelvic packing that has been described in the literature has consistently involved intraperitoneal packing. However, packing of the peritoneal cavity is often insufficient tamponade for bleeding associated with retroperitoneal and endometrial bleeding. Direct compression in the retroperitoneal space stanches bleeding from the iliac vessels and branches. In trauma, this technique is used to provide quick relief of pelvic hemorrhage in any setting, including the emergency and operating rooms.9-11
Technique
Retroperitoneal packing consists of a few basic steps and can be easily reproduced and applied in life-threatening circumstances. First, a 5-cm incision is made just cephalad to the symphysis pubis deep to the fascia and into the space of Retzius (FIGURE 1). The buildup of blood often causes autodissection of this plane (FIGURE 4). It is often useful to keep this fascial incision separate from the laparotomy fascial incision to assist with tamponade. Next, blunt dissection is performed in the continuous space of Retzius and retroperitoneum to the level of the presacral space (FIGURE 2).
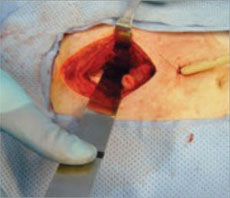
FIGURE 4 Expect autodissection
Blood loss frequently causes autodissection of the surgical plane. Tamponade is then achieved by placing laparotomy sponges into the retroperitoneal space (FIGURE 3). Packing with two or three laparotomy sponges at each side of the retroperitoneal pelvis is usually sufficient. In emergent situations, this entire procedure can be completed in an emergency room or postanesthesia care unit, with a drain left in place along with the packs (FIGURE 5). In trauma, this technique allows immediate stabilization of the patient until the underlying injury can be thoroughly addressed. Careful examination of the ureters and bladder should be completed to address any injury promptly.

FIGURE 5 A drain may be required
Packing can be left in place until bleeding is stanched, with a drain added for optimal recovery. The success of this technique is clear from the trauma literature, but the data have yet to be widely applied in nontraumatic applications.9 It is especially advantageous to have a space separate from the intraperitoneal cavity to provide tamponade because the uterus itself may obstruct visualization. It is possible that, in some cases, this technique may control bleeding without the need for postpartum hysterectomy.
CASE RESOLVED
When the retroperitoneal packs are removed after the hysterectomy, no further bleeding occurs. However, moderate hydronephrosis is apparent along the patient’s left ureter.
The wound is closed, and the patient is transferred to intensive care. She subsequently undergoes placement of a ureteral stent for the hydronephrosis and is discharged 5 days later. The stent is removed on an outpatient basis without further morbidity or the need for additional procedures.
Pelvic hemorrhage is a devastating complication in both trauma and postpartum situations. Postpartum hemorrhage complicates 6% of cesarean deliveries and leads to hysterectomy in 0.35 of every 1,000 deliveries. Maternal mortality approaches 13.6% in developing nations and 4% in industrialized nations.12
When does bleeding after delivery become “hemorrhage”?
Postpartum hemorrhage is often defined as more than 500 cc of blood loss after vaginal delivery or more than 1,000 cc during a cesarean delivery.13 Postpartum hemorrhage can be further classified into primary or secondary, depending on the timing of occurrence. Primary hemorrhage occurs within 24 hours of delivery; secondary hemorrhage occurs from 24 hours to 12 weeks after delivery.14
Causes of postpartum hemorrhage include uterine atony, retained placental products, genital laceration, inversion of the uterus, and coagulation disorders.