Injury-free vaginal surgery: Case-based protective tactics






A strategy for avoiding, recognizing, and repairing injuries intraoperatively—and averting litigation
IN THIS ARTICLE
If suture removal fails to bring about ureteral efflux, evaluate the ureters further by using intraoperative retrograde ureterogram (pyelogram) under fluoroscopy or by placing ureteral stents under cystoscopic guidance. Either method will localize the obstruction or kink and allow for targeted exploration and release of the stricture.
Extended bladder drainage is usually not required after intraoperative release of a partially or completely obstructed ureter.
In my practice, I remove any permanent suture I suspect is kinking or partially kinking a ureter. If the suture causing the problem is an absorbable one (eg, as in the use of Vicryl suture at colpocleisis), I may choose to follow the patient or to place a stent, and I reassure the woman that the offending suture will dissolve over time, thus relieving the partial obstruction.
If blue dye enters the field from inside the pelvis
The problem may be partial or complete ureteral transection. In this case, bladder perforation must first be ruled out cystoscopically. Then perform retrograde ureterogram under fluoroscopy to look for the possible point of leakage.
If ureteral transection is confirmed, plan for thorough surgical exploration (usually via the abdominal route) to locate and repair the injury.
For many generalists, this may require an intraoperative consult from a surgical service comfortable with the repair and/or reimplantation of the ureters.
CASE 1 OUTCOME
The bladder laceration was repaired after completion of the vaginal hysterectomy in the manner described above. There were no further sequelae.
It pays to refamiliarize yourself with the particular “landscape” of the lower urinary tract, so that sutures or scalpels don’t inadvertently block or injure structures.
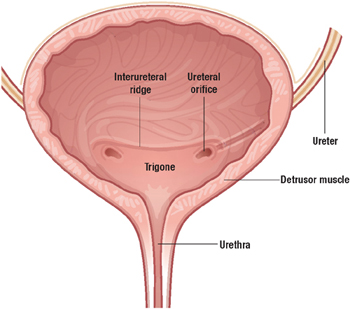
The smooth muscle of the bladder (detrusor) is lined with transitional mucosal epithelium and opens into the urethra at the bladder neck.
The ureters enter into the lateral aspects of the midposterior bladder and tunnel medially through the detrusor muscle before entering the bladder lumen at the level of the interureteral ridge. These entry points are known as the ureteral orifices.
The trigone is an area of the posterior bladder wall bounded by the bladder neck inferiorly and by the 2 ureteral orifices in the posterior midbladder.
Rectal injuries are usually easy to identify
As far as vaginal surgery is concerned, the lower GI tract consists of the rectum and external and internal anal sphincters. The distal rectum and posterior vaginal wall are usually closely applied to each other, separated by the rectovaginal septum (also called Denonvilliers fascia).
Risk factors
In women who have undergone posterior colporrhaphy or repair of a 4th degree tear, the posterior vaginal wall can be densely adherent to the rectum, putting the rectum at risk for injury during posterior vaginal wall dissection.
Most injuries to the rectum occur during dissection of the posterior vaginal wall. Fortunately, these injuries are readily recognized and easily repaired. If a rectal injury is suspected during or after dissection, a thorough intraoperative digital exam will help confirm or rule it out.
Repair of a rectal injury
Once an injury is identified, reapproximate the rectal mucosal edges with an imbricating closure using 3-0 Monocryl or other absorbable monofilament suture. A second imbricating layer should bring the rectal muscularis together, and the rectovaginal septum can then be closed over this layer in side-to-side or transverse fashion. Finally, close the vaginal mucosa after appropriate posterior colporrhaphy trimming. Such repairs heal well over time, without any long-term effects for the patient.
Prescribe a stool softener for the first 3 postoperative months to reduce the patient’s need to strain.
No bowel prep needed because injuries are rare
In my practice, the vast majority of vaginal surgical cases are accomplished without the need for preoperative bowel preparation. In the occasional patient known to have dense small-bowel adhesions involving the uterus, adnexae, or vaginal cuff, bowel prep may be appropriate if substantial dissection of the bowel is anticipated as part of the procedure.
CASE 2 Small bowel laceration
A 45-year-old woman with 4 prior vaginal deliveries, a 4th-degree obstetric rectovaginal laceration, and a history of laparoscopically assisted vaginal hysterectomy presents with stage III pelvic organ prolapse, primarily involving the posterior vaginal wall. An examination reveals a defect in the upper aspect of the posterior wall (an apical defect).
Intraoperatively, during sharp dissection to lift the posterior vaginal wall off the rectovaginal septum, a loop of small bowel descends into the field, and a 1-cm laceration occurs, exposing the lumen of the bowel.
How do you proceed?
On very rare occasions, a patient with an enterocele may sustain a small bowel injury during vaginal surgery. Such injury can usually be avoided by packing the small bowel away from the area of dissection and closely observing the dissection field.