Barriers and Facilitators to Guideline-Adherent Pulse Oximetry Use in Bronchiolitis





OBJECTIVE: Continuous pulse oximetry monitoring (cSpO2) in children with bronchiolitis does not improve clinical outcomes and has been associated with increased resource use and alarm fatigue. It is critical to understand the factors that contribute to cSpO2 overuse in order to reduce overuse and its associated harms.
METHODS: This multicenter qualitative study took place in the context of the Eliminating Monitor Overuse (EMO) SpO2 study, a cross-sectional study to establish rates of cSpO2 in bronchiolitis. We conducted semistructured interviews, informed by the Consolidated Framework for Implementation Research, with a purposive sample of stakeholders at sites with high and low cSpO2 use rates to identify barriers and facilitators to addressing cSpO2 overuse. Interviews were audio recorded and transcribed. Analyses were conducted using an integrated approach.
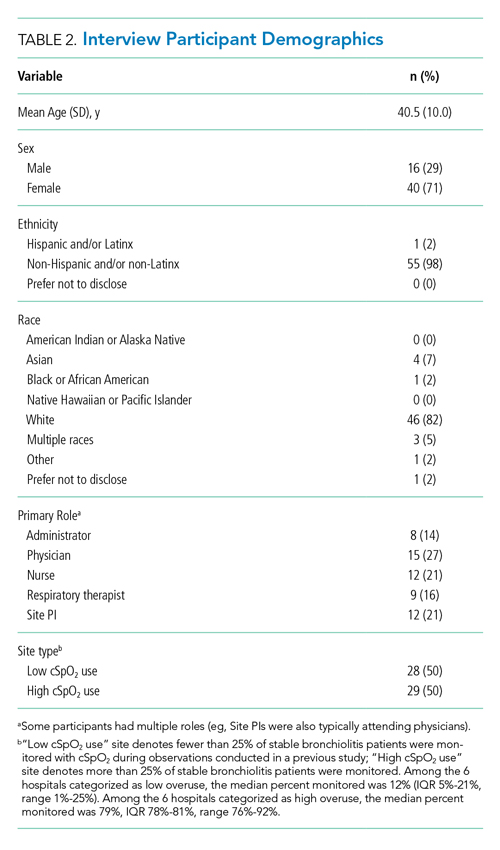
RESULTS: Participants (n = 56) included EMO study site principal investigators (n = 12), hospital administrators (n = 8), physicians (n = 15), nurses (n = 12), and respiratory therapists (n = 9) from 12 hospitals. Results suggest that leadership buy-in, clear authoritative guidelines for SpO2 use incorporated into electronic order sets, regular education about cSpO2 in bronchiolitis, and visual reminders may be needed to reduce cSpO2 utilization. Parental perceptions and individual clinician comfort affect cSpO2 practice.
CONCLUSION: We identified barriers and facilitators to deimplementation of cSpO2 for stable patients with bronchiolitis across children’s hospitals with high- and low-cSpO2 use. Based on these data, future deimplementation efforts should focus on clear protocols for cSpO2, EHR changes, and education for hospital staff on bronchiolitis features and rationale for reducing cSpO2.
© 2021 Society of Hospital Medicine
Procedure
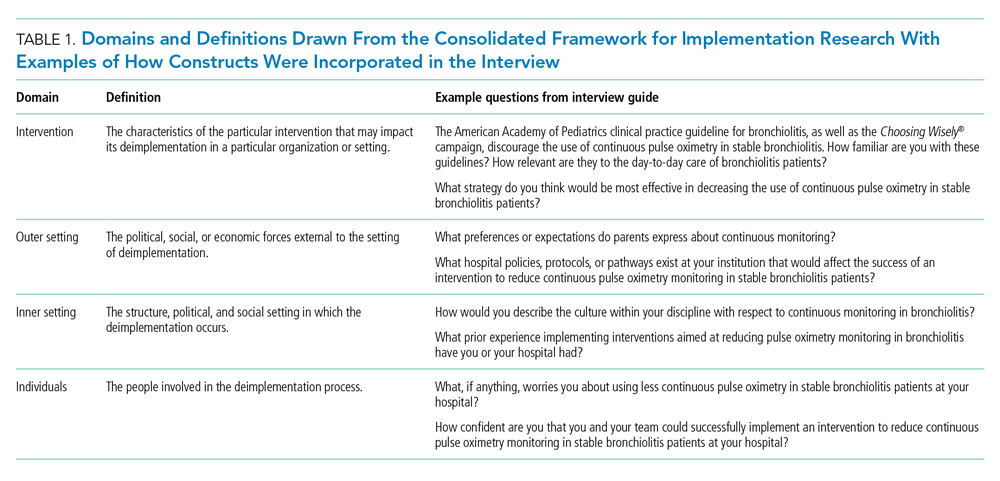
The interview guide was informed by the CFIR, a comprehensive framework detailing contextual factors that require consideration when planning for the implementation of a health service intervention. Table 1 details the CFIR domains with study-related examples. The interview guide (Appendix) provided limited clinical context apart from the age, diagnosis, and oxygen requirement for the population of interest to promote a broad array of responses and to avoid anchoring on specific clinical scenarios. Interviews were conducted by master’s degree or doctoral-level research coordinators with qualitative interviewing experience and supervised by a medical anthropologist and qualitative methods expert (F.K.B.). Prior to engaging in audio recorded phone interviews, the interviewer explained the risks and benefits of participating. Participants were compensated $50. Audio recordings were transcribed, deidentified, and uploaded to NVivo 12 Plus (QSR International) for data management.
The Institutional Review Boards of Children’s Hospital of Philadelphia, Pennsylvania, and the University of Pennsylvania in Philadelphia determined that the study met eligibility criteria for IRB exemption.
Data Analysis
Using an integrated approach to codebook development,26 a priori codes were developed using constructs from the CFIR. Additional codes were added by the research team following a close reading of the first five transcripts.27,28 Each code was defined, including decision rules for its application. Two research coordinators independently coded each transcript. Using the intercoder reliability function within NVivo, the coders established strong interrater reliability accordance scores (
RESULTS
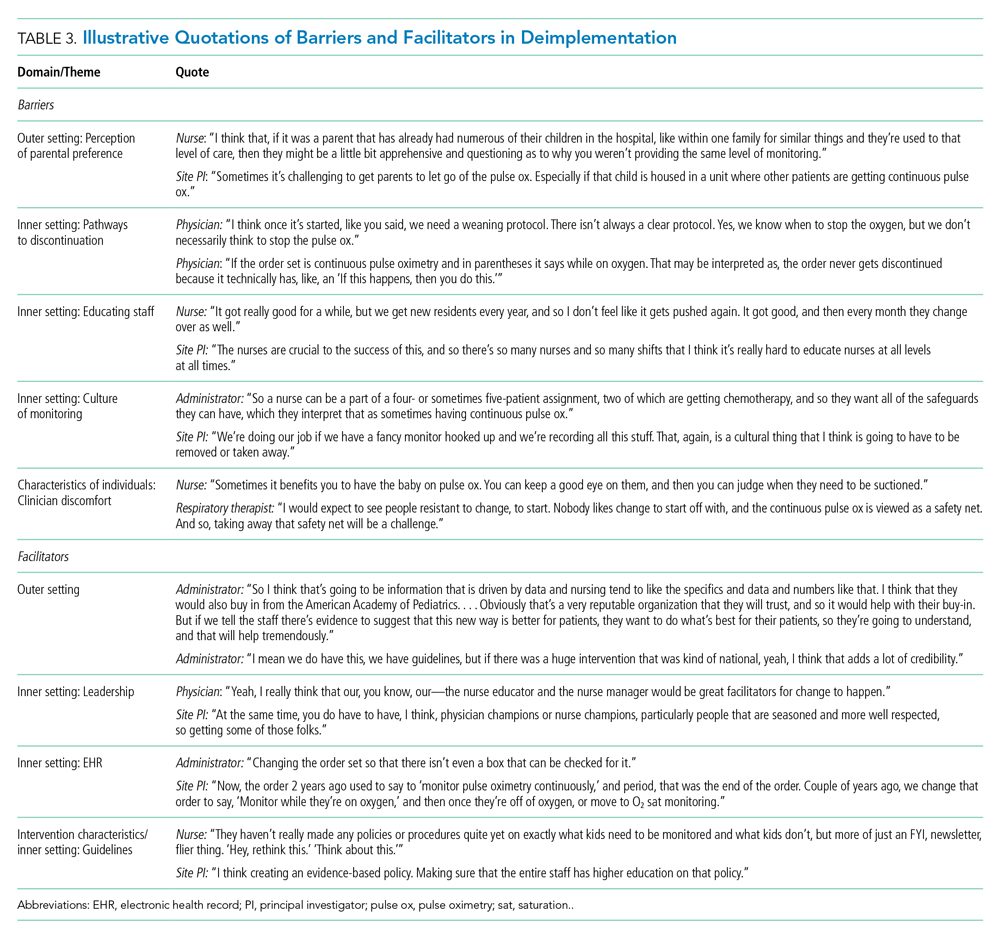
Barriers and facilitators to deimplementation were identified in multiple domains of the CFIR: outer setting, inner setting, characteristics of the individuals, and intervention characteristics (Table 1). Participants also suggested strategies to facilitate deimplementation in response to some identified barriers. See Table 2 for participant demographics and Table 3 for illustrative participant quotations.
Barriers
Outer Setting: Clinician Perceptions of Parental Discomfort With Discontinuing Monitoring
Participants mentioned parental preferences as a barrier to discontinuing cSpO2, noting that parents seem to take comfort in watching the numbers on the monitor screen and are reluctant to have it withdrawn. Clinicians noted that parents sometimes put the monitor back on their child after a clinician removed it or have expressed concern that their unmonitored child was not receiving the same level of care as other patients who were being monitored. In these scenarios, clinicians reported they have found it helpful to educate caregivers about when cSpO2 is and is not appropriate.
Inner Setting: Unclear or Nonexistent Guideline to Discontinue cSpO2
Guidelines to discontinue cSpO2 reportedly did not exist at all institutions. If a guideline did exist, lack of clarity or conflicting guidelines about when to use oxygen presented a barrier. Participants suggested that a clear guideline or additional oversight to ensure all clinicians are informed of the procedure for discontinuing cSpO2 may help prevent miscommunication. Participants noted that their electronic health record (EHR) order sets commonly included cSpO2 orders and that removing that option would facilitate deimplementation.
