Hospital Medicine Management in the Time of COVID-19: Preparing for a Sprint and a Marathon





© 2020 Society of Hospital Medicine
The pandemic of coronavirus disease 2019 (COVID-19) is confronting the modern world like nothing else before. With over 20 million individuals expected to require hospitalization in the US, this health crisis may become a generation-defining moment for healthcare systems and the field of hospital medicine.1 The specific challenges facing hospital medicine are comparable to running a sprint and a marathon—at the same time. For the sprint underway, hospitalists must learn to respond to a rapidly changing environment in which critical decisions are made within hours and days. At the same time, hospitalists need to plan for the marathon of increased clinical needs over the coming months, the possibility of burnout, and concerns about staff well-being. Although runners typically focus on either the sprint or the marathon, healthcare systems and hospital medicine providers will need to simultaneously prepare for both types of races.
GET READY FOR THE SPRINT
Over the past several weeks, hospital medicine leaders have been rapidly responding to an evolving crisis. Leaders and clinicians are quickly learning how to restructure clinical operations, negotiate the short supply of personal protective equipment (PPE), and manage delays in COVID-19 testing. In these areas, our hospitalist group has experienced a steep learning curve. In addition to the strategies outlined in the Table, we will share here our experiences and insights on managing and preparing for the COVID-19 pandemic.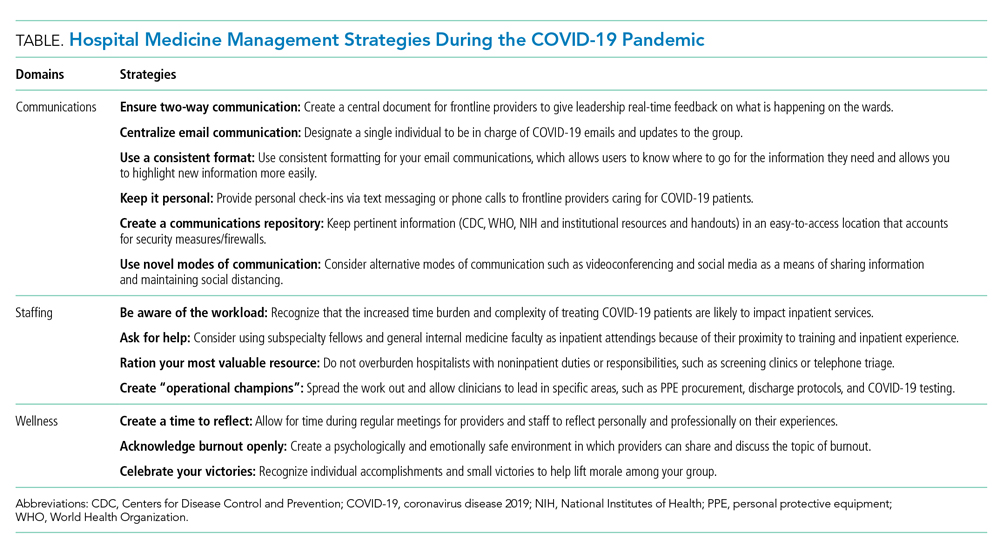
Communication Is Central
During the sprint, focused, regular communication is imperative to ameliorate anxiety and fear. A study of crisis communication after 9/11 found that, for employees, good communication from leadership was one of the most valued factors.2 Communications experts also note that, in times of crisis, leaders have a special role in communication, specifically around demystifying the situation, providing hope, and maintaining transparency.3
Mental bandwidth may be limited in a stressful environment, so efforts should be taken to maximize the value of each communication. Information on hospital metrics should be provided regularly, including the number of COVID-19 cases, the status of clinical services and staffing, hospital capacity, and resource availability.4 Although the ubiquity and ease of email is convenient, recognize that providers are likely receiving email updates from multiple layers within your healthcare organization. To guard against losing important information, we use the same templated format for daily email updates with changes highlighted, which allows busy clinicians to digest pertinent information easily.5 Finally, consider having a single individual be responsible for collating COVID-19–related emails sent to your group. Although clinicians may want to share the most recent studies or their clinical experiences with a group email, instead have them send this information to a single individual who can organize these materials and share them on a regular basis.
To keep two-way communication channels open in a busy, asynchronous environment, consider having a centralized shared document in which providers can give real-time feedback to capture on-the-ground experiences or share questions they would like answered. Within our group, we found that centralizing our conversation in a shared document eliminated redundancy, focused our meetings, and kept everyone up to date. Additionally, regularly scheduled meetings may need to be adapted to a remote format (eg, Zoom, WebEx) as clinicians are asked to work from home when not on clinical service. Finally, recognize that virtual meetings require a different skill set than that required by in-person meetings, including reestablishment of social norms and technology preparation.6