Social Disadvantage, Access to Care, and Disparities in Physical Functioning Among Children Hospitalized with Respiratory Illness





BACKGROUND AND OBJECTIVES: Understanding disparities in child health-related quality of life (HRQoL) may reveal opportunities for targeted improvement. This study examined associations between social disadvantage, access to care, and child physical functioning before and after hospitalization for acute respiratory illness.
METHODS: From July 1, 2014, to June 30, 2016, children ages 8-16 years and/or caregivers of children 2 weeks to 16 years admitted to five tertiary care children’s hospitals for three common respiratory illnesses completed a survey on admission and within 2 to 8 weeks after discharge. Survey items assessed social disadvantage (minority race/ethnicity, limited English proficiency, low education, and low income), difficulty/delays accessing care, and baseline and follow-up HRQoL physical functioning using the Pediatric Quality of Life Inventory (PedsQL, range 0-100). We examined associations between these three variables at baseline and follow-up using multivariable, mixed-effects linear regression models with multiple imputation sensitivity analyses for missing data.
RESULTS: A total of 1,325 patients and/or their caregivers completed both PedsQL assessments. Adjusted mean baseline PedsQL scores were significantly lower for patients with social disadvantage markers, compared with those of patients with none (78.7 for >3 markers versus 85.5 for no markers, difference −6.1 points (95% CI: −8.7, −3.5). The number of social disadvantage markers was not associated with mean follow-up PedsQL scores. Difficulty/delays accessing care were associated with lower PedsQL scores at both time points, but it was not a significant effect modifier between social disadvantage and PedsQL scores.
CONCLUSIONS: Having social disadvantage markers or difficulty/delays accessing care was associated with lower baseline physical functioning; however, differences were reduced after hospital discharge.
© 2020 Society of Hospital Medicine
Social Disadvantage Markers and PedsQL Scores
The number of social disadvantage markers was inversely related to mean baseline PedsQL scores, but there was no difference in mean follow-up PedsQL scores between social disadvantage groups (Table 2). In adjusted analyses, the mean baseline PedsQL score was −6.1 points (95% CI: −8.7, −3.5) lower for patients with >/= 3 social disadvantage markers compared with patients with no social disadvantage markers, which exceeded the scale’s MCID.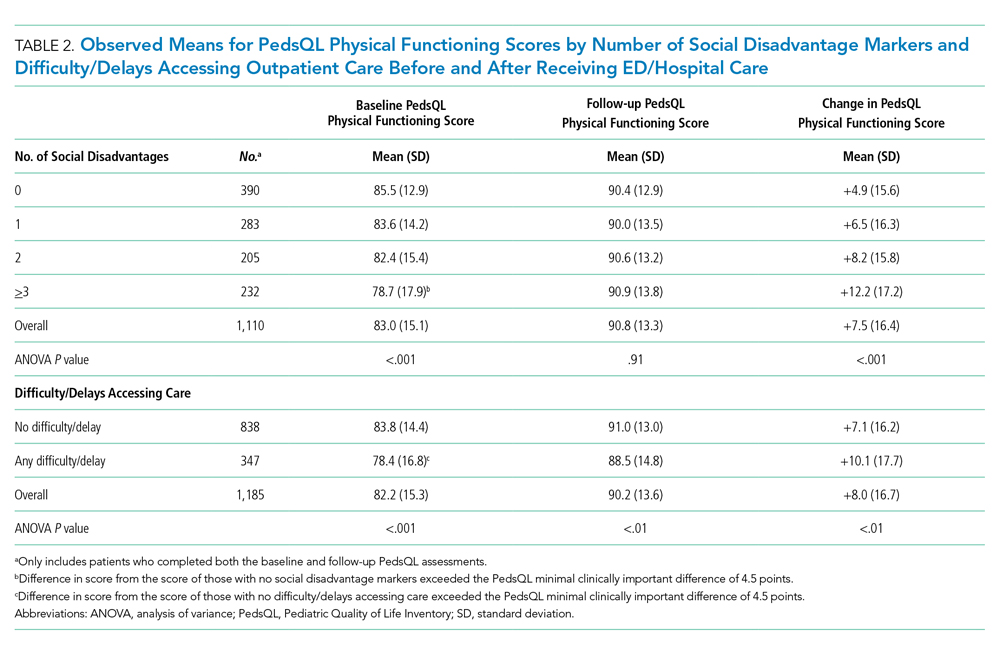
Difficulty/Delays Accessing Care and PedsQL Scores
Having any difficulty/delays accessing care was significantly associated with lower baseline and follow-up PedsQL scores (Table 2). In adjusted analyses, the difference in baseline scores was 5.2 points (95% CI: −7.2, −3.2), which exceedes the scale’s MCID.
Interaction Between Social Disadvantage Markers, Difficulty/Delays Accessing Care, and Change in PedsQL Scores from Baseline to Follow-Up
While having =/>2 social disadvantage markers and difficulty/delays accessing care were each positively associated with changes in PedsQL scores from baseline to follow-up (Table 3), only patients with =/> 3 social disadvantage markers exceeded the PedsQL MCID. In stratified analyses, patients with a combination of social disadvantage makers and difficulties/delays accessing care had lower baseline PedsQL scores and greater change in PedsQL scores from baseline to follow-up compared with those without difficulties/delays accessing care (Figure). However, having any difficulty/delays accessing care did not significantly modify the relationship between social disadvantage and change in PedsQL scores, as none of the interaction terms were significant (Table 3, Model 3).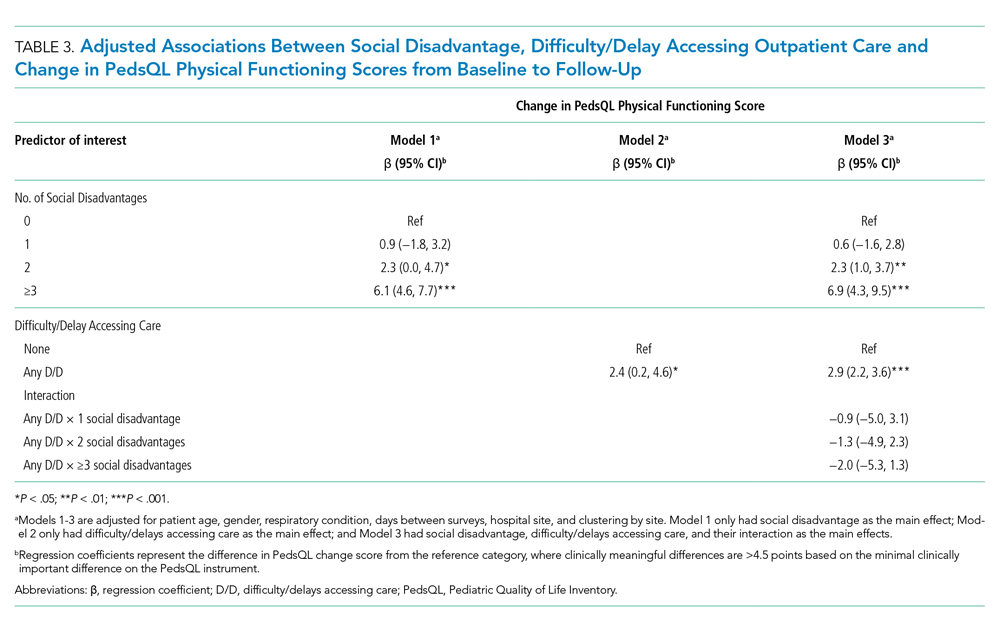
Sensitivity Analysis
Baseline, follow-up, and change in PedsQL scores were similar to our main analysis after performing multiple imputation for missing social disadvantage markers (Supplemental Table 1). Findings were also similar for patients with a diagnosis of asthma only; however, changes in PedsQL scores were greater in magnitude (Appendix Table 2).
DISCUSSION
This study examined the relationship between social disadvantage and child physical functioning before and after hospitalization for acute respiratory illness. Study findings indicated that patients with higher numbers of social disadvantage markers reported lower PedsQL scores before hospitalization; however, differences in PedsQL scores were not apparent after hospitalization. Patients who experienced difficulty/delays accessing care also reported lower PedsQL scores at baseline. This difference was still significant but did not exceed the PedsQL MCID threshold after hospitalization. Difficulty/delays accessing care appeared to be an additional social disadvantage marker; however, it did not modify the relationship between social disadvantage and improvement in physical functioning.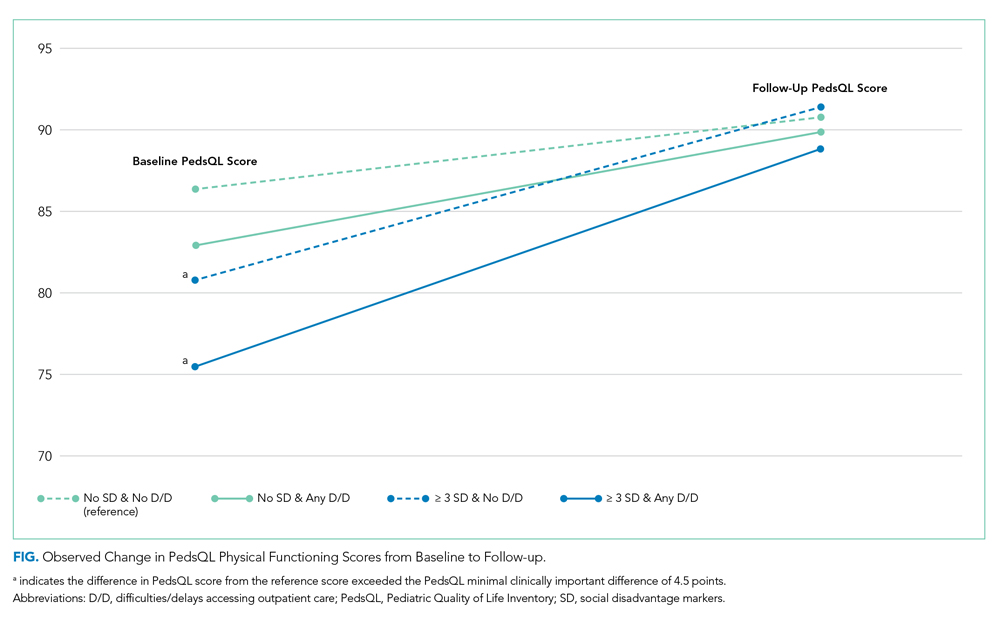
The study findings at baseline are consistent with prior studies demonstrating a negative association between social disadvantage markers and HRQoL and a cumulative effect based on the number of social disadvantages.3,4,7,8 This study adds to the existing literature by examining how this relationship changes after hospitalization. As evidenced by the lack of association between social disadvantage markers and follow-up PedsQL scores, our findings suggest that receipt of inpatient care improved perceptions of physical functioning to a greater extent for patients with more social disadvantage markers (especially patients with =/> 3 social disadvantage markers). There are several potential reasons for these findings.
