New Answers for Old Questions in the Treatment of Severe Infections from Injection Drug Use





Hospitalists are increasingly responsible for the management of infectious consequences of opioid use disorder (OUD), including increasing rates of hospitalization for injection drug use (IDU)-associated infective endocarditis, osteomyelitis, and soft tissue infections. Management of IDU-associated infections poses unique challenges: symptoms of the underlying addiction can interfere with care plans, patients often have difficult psychosocial circumstances in addition to their addiction, and they are often stigmatized by the healthcare system. Although there are few randomized trial data to support one particular approach to management, the literature suggests that successful treatment of IDU-associated infections requires appropriate antimicrobial and surgical interventions in addition to acknowledgment and treatment of the underlying OUD. In this narrative review, the best available evidence is used to answer several of the most commonly encountered questions in the management of IDU-associated infections. These data are used to develop a framework for hospitalists to approach the care of patients with IDU-associated infections.
© 2019 Society of Hospital Medicine
As a result of the epidemic of opioid use disorder (OUD), there has been a secondary surge in hospitalizations for infectious complications of injection drug use (IDU).1,2 In the previous 10 years, there have been significant increases in IDU-associated human immunodeficiency virus (HIV)3 and hepatitis C virus (HCV)4 infection as well as increased hospitalizations from IDU-associated skin and soft tissue infections, osteomyelitis, septic arthritis, bacteremia, fungemia, and infective endocarditis in the United States.2,5-7 Patients admitted with IDU-associated infections have long lengths of stay, high rates of leaving against medical advice (AMA), readmission, and mortality.8-13 In a British cohort (median age 36 years), five-year mortality after an episode of IDU-associated endocarditis was 42%.14 Admissions for IDU-associated infections can be a troubling experience for both patients and providers alike.15 While management decisions of IDU-associated infectious syndromes have sometimes been based on emotion, dogma, and an often-stigmatizing approach toward people suffering from addiction,16 with a better understanding of addiction and effective treatments, as well as accumulating data in both addiction and infectious disease fields, it is an appropriate time to reevaluate the approach to treatment.
The goal of this review is to examine recent evidence and attempt to answer questions that frequently arise in the management of hospitalized patients with IDU-associated infections
KEY MANAGEMENT QUESTIONS IN THE INPATIENT MANAGEMENT OF INFECTIOUS COMPLICATIONS OF OUD
How Should OUD Be Managed in the Hospital?
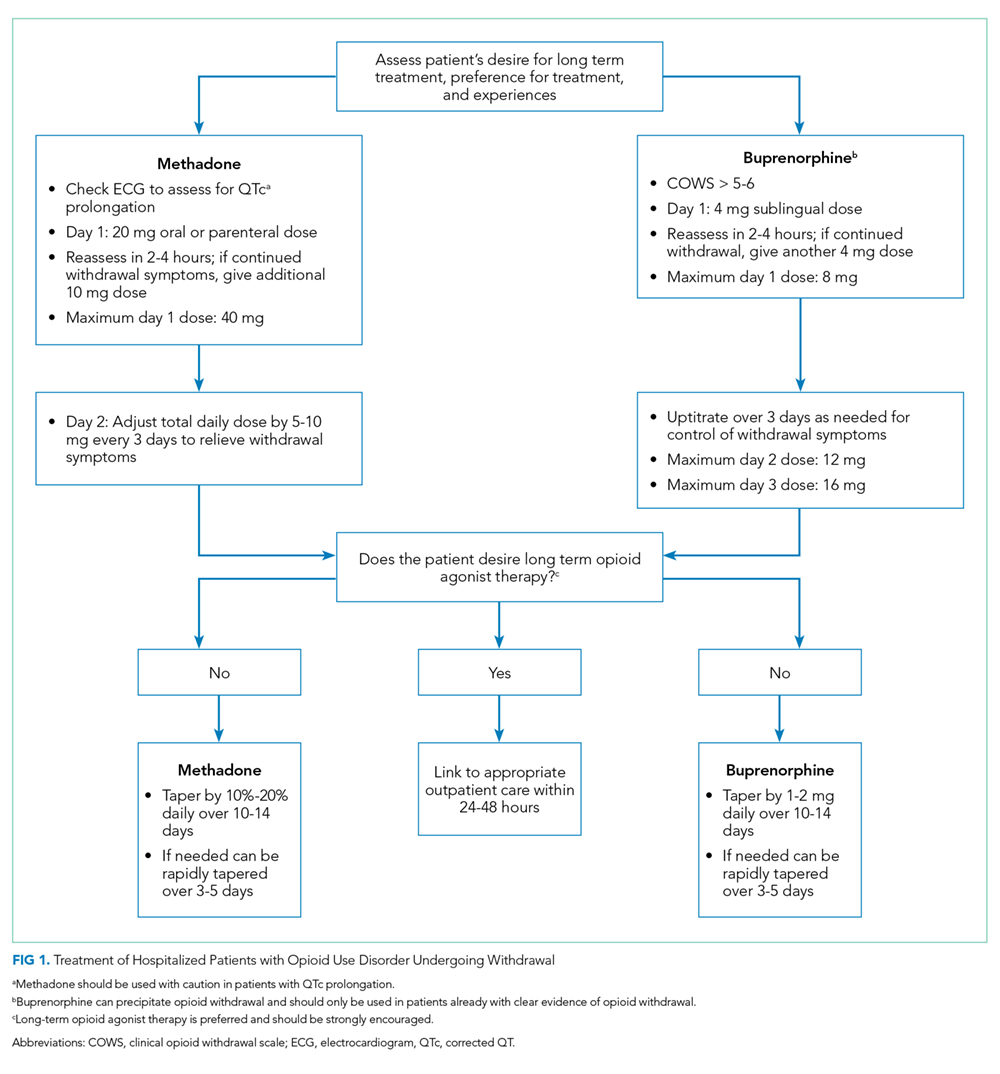
Management of an IDU-associated infection is incomplete without addressing the underlying addiction in some way. Addiction is highly undertreated among patients with IDU-associated infections, which may contribute to poor infection-related outcomes.8,13,17 Opioid agonist therapy (buprenorphine and methadone) to prevent withdrawal should be routinely offered to all patients with OUD including those with infectious complications of OUD to facilitate appropriate medical treatment and engage patients in long-term addiction treatment. Referral to addiction treatment has been associated with improved IDU-associated endocarditis mortality,18 and initiation of medications for OUD (MOUD) can be achieved successfully in the emergency department, inpatient wards, and specifically in patients admitted with IDU-associated endocarditis.19-21 Protocols and resources for inpatient management of withdrawal and initiation of MOUD are available along with telephone support services for providers seeking guidance on specific cases.21,22 Inpatient addiction consult services are an important resource for the management of hospitalized patients with addiction and are associated with increased completion of antibiotics, decreased AMA discharge, and increased rates of MOUD provision among patients with IDU-associated infections.12 However, when unavailable, initiation of opioid agonist therapy does not require an addiction specialist. Linkage to outpatient addiction care is ideal; however, opioid agonist therapy initiated in the hospital can be tapered prior to discharge if this is unavailable. Figure 1 outlines the initiation of methadone or buprenorphine for the treatment of both withdrawal and OUD in the inpatient setting.20,21