A Time Motion Study Evaluating the Impact of Geographic Cohorting of Hospitalists





BACKGROUND: Geographic cohorting (GCh) localizes hospitalists to a unit. Our objective was to compare the GCh and non-GCh workday.
METHODS: In an academic, Midwestern hospital we observed hospitalists in GCh and non-GCh teams. Time in patient rooms was considered direct care; other locations were considered ‘indirect’ care. Geotracking identified time spent in each location and was obtained for 17 hospitalists. It was supplemented by in-person observation of four GCh and four non-GCh hospitalists for a workday each. Multilevel modeling was used to analyze associations between direct and indirect care time and team and workday characteristics.
RESULTS: Geotracking yielded 10,522 direct care episodes. GCh was associated with longer durations of patient visits while increasing patient loads were associated with shorter visits. GCh, increasing patient loads, and increasing numbers of units visited were associated with increased indirect care time. In-person observations yielded 3,032 minutes of data. GCh hospitalists were observed spending 56% of the day in computer interactions vs non-GCh hospitalists (39%; P < .005). The percentage of time spent multitasking was 18% for GCh and 14% for non-GCh hospitalists (P > .05). Interruptions were pervasive, but the highest interruption rate of once every eight minutes in the afternoon was noted in the GCh group.
CONCLUSION: GCh may have the potential to increase patient–hospitalist interactions but these gains may be attenuated if patient loads and the structure of cohorting are suboptimal. The hospitalist workday is cognitively intense. The interruptions noted may increase the time taken for time-intensive tasks like electronic medical record interactions.
© 2019 Society of Hospital Medicine
RESULTS
Locator Badge Observations
Participants
The 17 hospitalists had a mean (SD) age of 38 years (6.4); 10 (59%) were male, 7 (41%) were international medical graduates, and 10 (59%) had worked at the hospital ≥5 years. The duration of observation was <45 days for 7 hospitalists, 46-55 days for 4, and >55 days for 6, yielding observations for 666 hospitalist workdays. The mean time since medical school graduation was 13 years. Seven hospitalists were observed only in the GCh model, one was observed only in the non-GCh model, and nine were observed in both.
Team Characteristics
On average, non-GCh teams visited more units per day than GCh teams. Teams with APPs had higher patient loads (Table 1).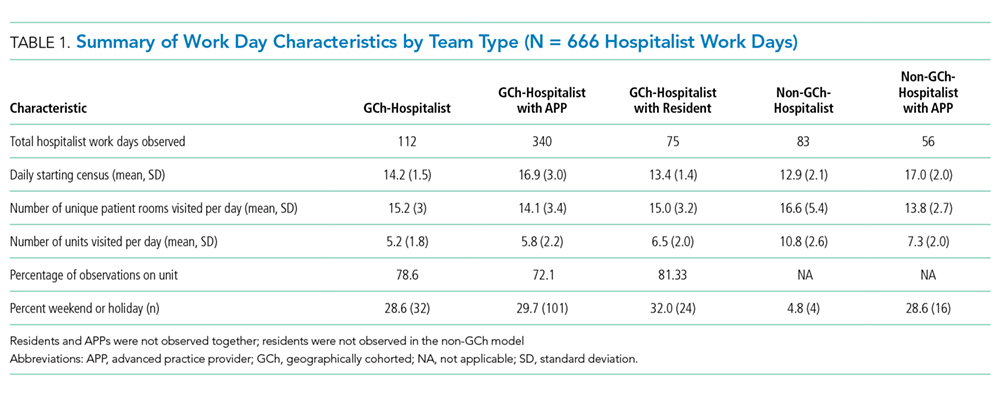
Time Observed in Direct and Indirect Care
In total, 10,522 observations were recorded in providing direct care. The average duration of a direct care encounter ranged from 4.1 to 5.8 minutes. The ratio of indirect to direct time ranged from 2.7 to 3.7 (Table 2).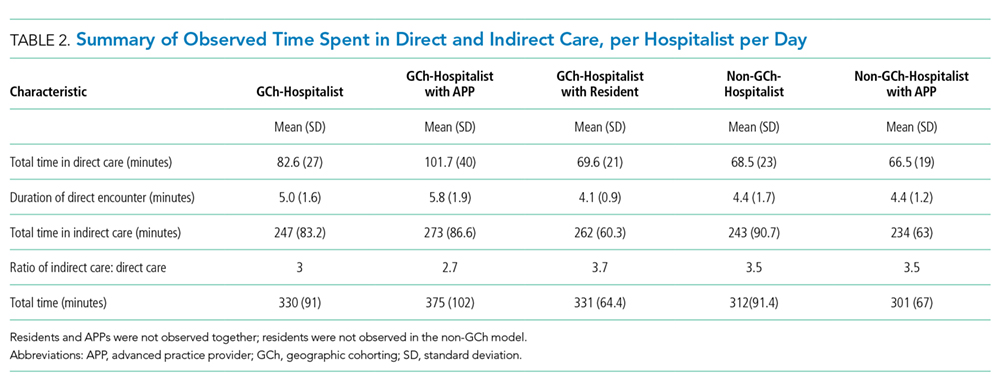
The number of times that a hospitalist visited the same patient room in one day ranged from 1 to 9. Most (84%) of the patient rooms were visited once per day. The odds that a GCh hospitalist would visit a patient more than once per day were 1.8 times higher (95% CI: 1.37, 2.34; P < .0001) than for a non-GCh hospitalist (data not shown).
Predictors Associated with Time Expenditure
Predictors significantly associated with both the duration of direct care encounters and total daily indirect care time included team type and patient count. Predicted time in direct care encounters was highest for the GCh-hospitalist team (9.5 minutes) and lowest for the GCh-hospitalist with residents team (7 minutes). Predicted total indirect care time was highest for the GCh-hospitalist with APP team (160 minutes) while the lowest expenditure in indirect care time was predicted for the non-GCh-hospitalist team (102 minutes). Increasing patient load from 10 to 20 was predicted to decrease the duration of a direct care encounter by one minute (14%) and increase the total indirect care time by a larger amount (39 min, 24%).
The duration of direct care encounters was also inversely related with years since medical school and number of visits made to same patient room. Finally, acuity of care was associated with the duration of direct care encounters with the longest predicted encounters in the ED (9.4 minutes). Physician gender and age, international graduation, years at current hospital, weekday, and the number of units visited in a day were neither associated with direct care time at P value < .05 nor improved model fit and therefore were not retained in the final model (Table 3).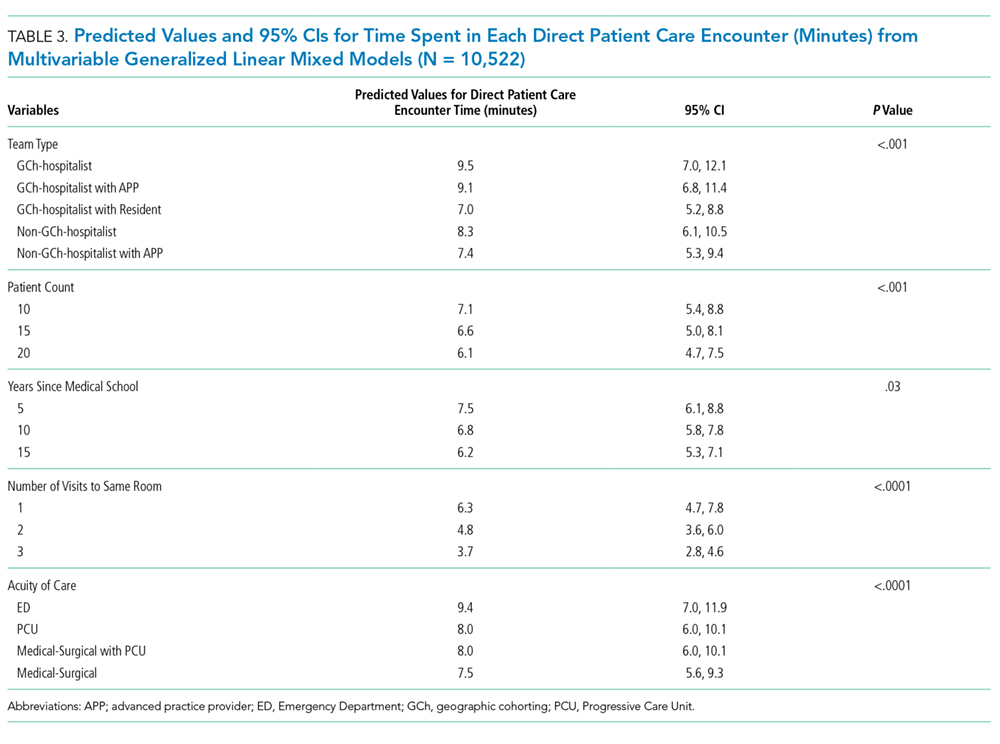
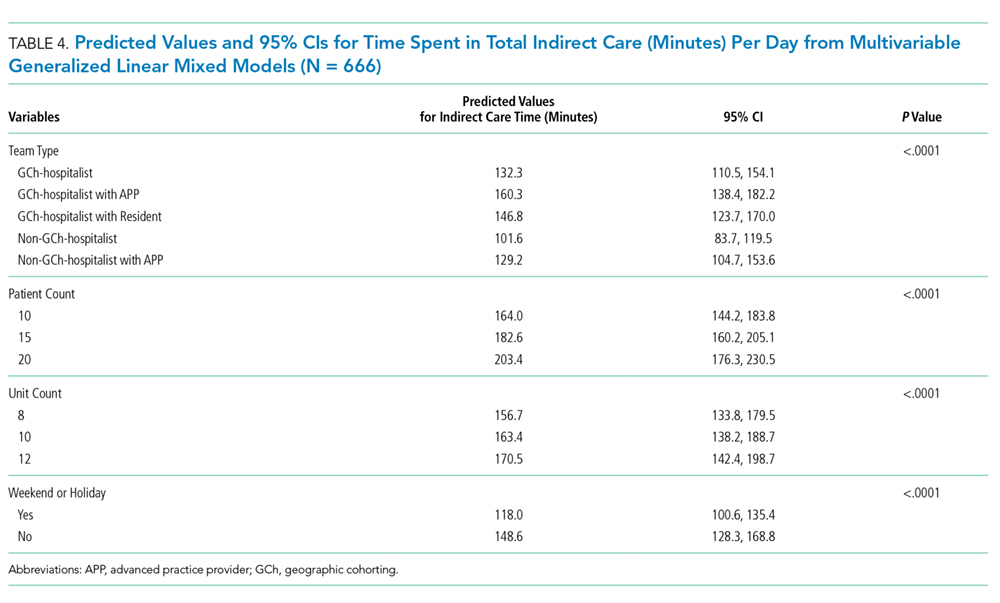
Additional predictors associated with total daily indirect care time included the number of units visited and working on a weekend or holiday. Total time spent in indirect care was predicted to increase as the number of units increased and decrease on weekends or holidays. Hospitalist characteristics were not associated with time in indirect care (Table 4).