Patient Safety Indicator-12 Rarely Identifies Problems with Quality of Care in Perioperative Venous Thromboembolism





BACKGROUND: Patient safety indicators (PSI) were developed for hospitals to screen for healthcare-associated adverse events. PSIs are believed to be preventable and have become a part of major pay-for-performance programs. PSI-12 captures perioperative venous thromboembolism (VTE), which contributes to morbidity and mortality of hospitalized patients. We aimed to evaluate PSI-12 events at our institution to identify areas for improvement of perioperative VTE prevention.
METHODS: We identified PSI-12 events from June 2015 to June 2017 using the Agency for Healthcare Research and Quality software version 5. Events were reviewed using our electronic medical record to identify further details of each event.
RESULTS: A total of 154 perioperative VTE cases were analyzed in the 2-year period. Pulmonary embolism (PE) occurred in 62.9% of cases, deep venous thrombosis (DVT) in 24%, and concurrent DVT/PE in 12.9%. The mean age of patients was 56 years old. Deficiencies in guideline-appropriate prophylaxis were identified in only 17 (11%) of cases. Unfractionated heparin was used in 61 cases, enoxaparin in 31 cases, and nine events occurred on therapeutic anticoagulation. Mechanical prophylaxis was used in 51 cases because of bleeding risk, thrombocytopenia, and/or liver associated coagulopathy. Four events occurred prior to the index procedure, with another eight cases occurring intraoperatively, or on the day of the procedure.
CONCLUSIONS: PSI-12 has several limitations in identifying quality of care issues in perioperative VTE. While it may be useful as a screening tool, further research for improvements are needed if it will remain one of the key measures in pay-for-performance.
© 2019 Society of Hospital Medicine
We considered perioperative VTE pharmacologic prophylaxis appropriate if started within 24 hours of a low bleeding risk procedure or 72 hours of a high-bleeding risk procedure.13 Mechanical prophylaxis was considered appropriate if pharmacologic prophylaxis was not used because of procedure risk, thrombocytopenia, or active bleeding. The medication administration record was reviewed to determine if prophylaxis was ordered, given, and/or refused.
RESULTS
During the two-year period, 18,084 surgeries were performed, and 161 cases of VTE events were identified. A detailed chart review and correction of documentation led to the exclusion of seven cases (4%) because the VTE event occurred prior to admission (n = 5) or were incidental findings that did not meet the Uniform Hospital Discharge Data Set definition for reporting (n = 2). In total, 154 (0.9% of all surgeries) cases were considered PSI-12 events. Pulmonary embolism (PE) occurred in most cases (n = 97, 62.9%), followed by deep vein thrombosis (DVT) (n = 37, 24.0%). Twenty cases (12.9%) experienced concurrent PE and DVT. Within the PE group, 16 cases (14%) were subsegmental PE only. Eight patients (14% of DVT cases) had only a distal DVT. The mean age of patients was 56 years (+/− 16 years), and the majority (59%) were male. The clinical specialties with the most events included neurosurgery (21%), orthopedics (14%), general surgery (13%), and trauma (11%). Fourteen patients (9%) died during the hospitalization, and of these, six (43%) had either sudden death or death attributed to PE (Table 1).
Cases were also reviewed for the type of VTE prophylactic strategy administered at the time of the event. The top three prophylactic strategies were subcutaneous unfractionated heparin (61%), mechanical prophylaxis only (51%), and enoxaparin (31%). Nine cases of VTE occurred during therapeutic anticoagulation (6%; Table 1).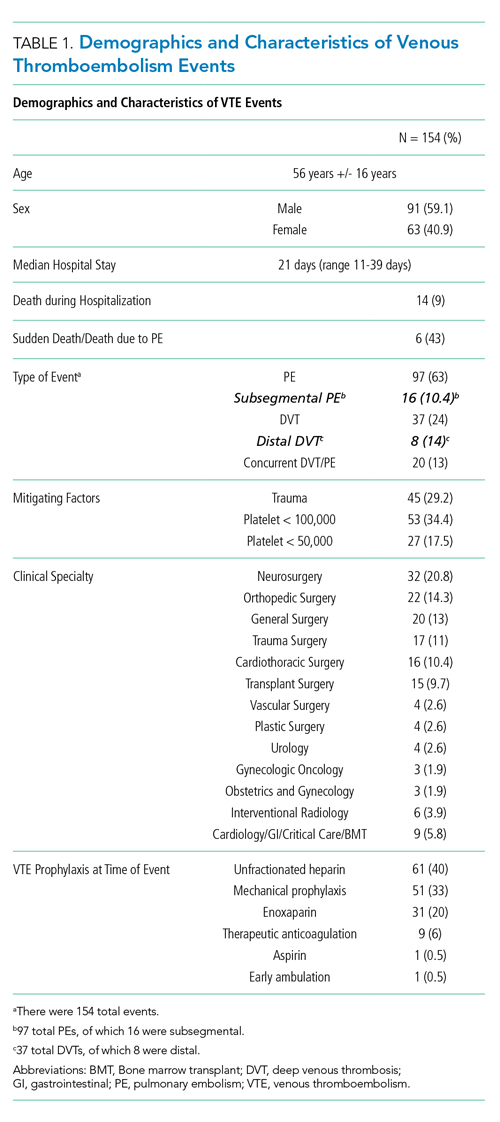
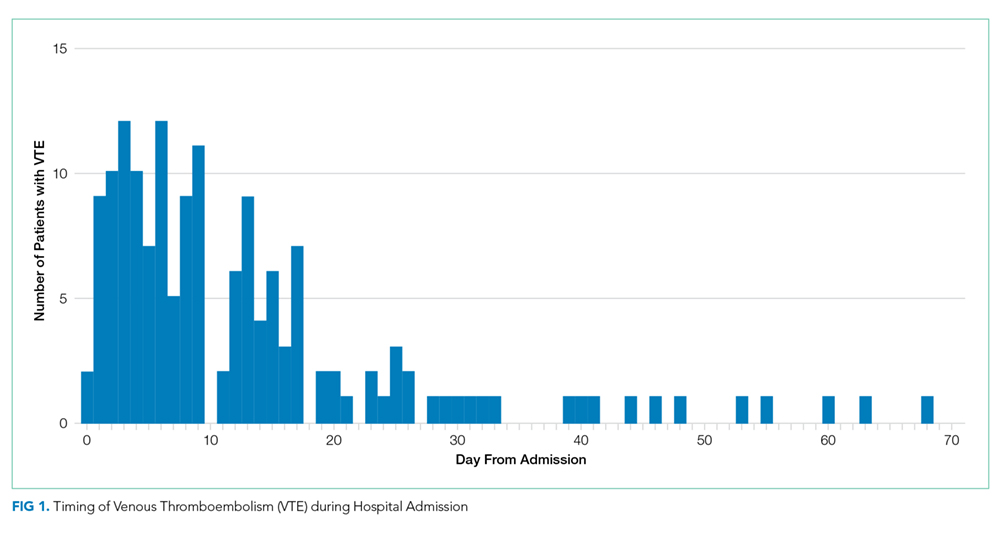
We also evaluated the timing of VTE in relation to hospitalization and procedure. Overall, the median length of hospital stay was 21 days (range: 11-39 days). VTE occurred early in the hospitalization; 21% of cases of VTE occurred within three days of admission, and 43.5% occurred within seven days of admission (Figure 1). With regard to VTE timing in relation to the procedure, 4.5% of cases of VTE occurred prior to the procedure, 33% occurred within three days of the procedure, and 53% occurred within seven days (Figure 2).
Absence of guideline-appropriate VTE prophylaxis was identified in only nine (6%) cases: seven patients had delayed initiation of pharmacologic prophylaxis, and two had pharmacologic prophylaxis held for unknown reasons. When accounting for pharmacologic prophylaxis missed based on patient refusal (n = 10 patients), the number of patients without guideline- appropriate VTE prophylaxis increased to 17 cases (11%), as two of the cases with patient refusal were found to have other quality issues present. Pharmacologic prophylaxis was given to 125 patients during their hospitalization. A median of 8% of ordered doses was refused, and an additional 8% of doses were held for a procedure (Table 2). We evaluated other factors that could have influenced the rate or type of VTE prophylactic strategies toward the use of mechanical prophylaxis, including thrombocytopenia and trauma. Although 11% of cases were treated primarily by the trauma teams (Table 1), a trauma-related procedure accounted for 29% of PSI-12 cases. Thrombocytopenia (platelets of less than 100,000) occurred in 53 cases (34%), with 27 patients (18%) having a platelet count of less than 50,000.