Prediction of Disposition Within 48 Hours of Hospital Admission Using Patient Mobility Scores





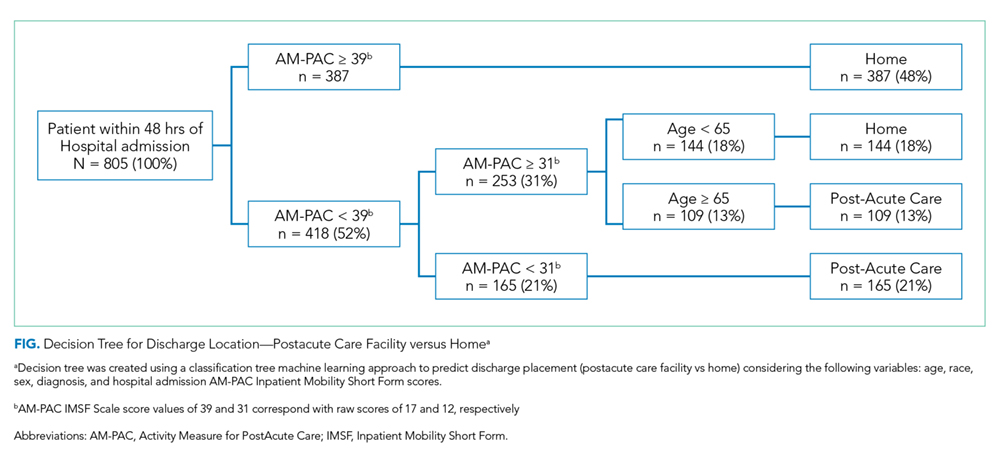
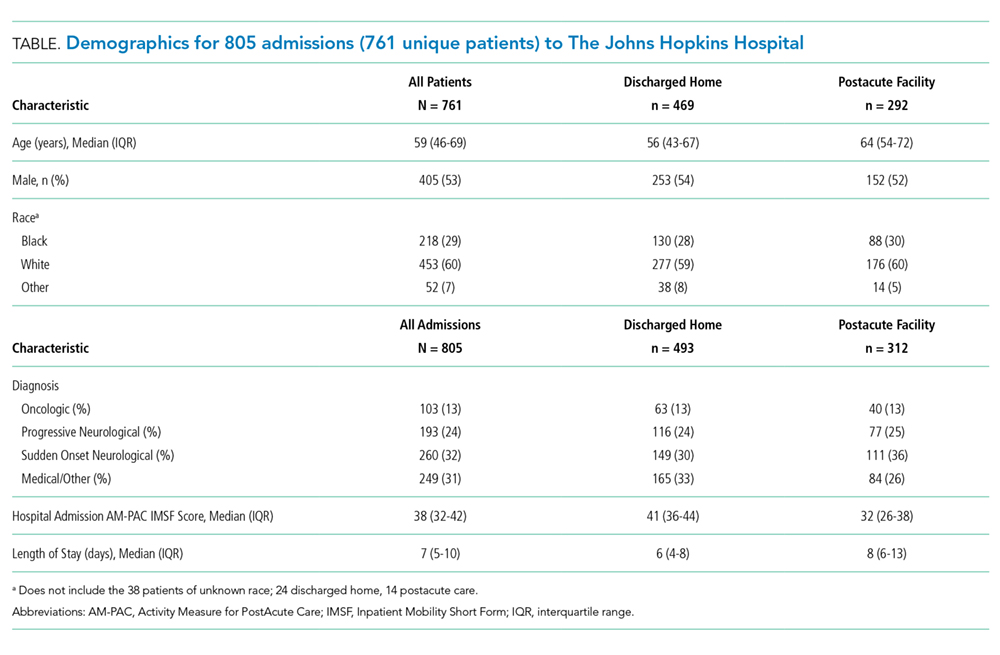
Delayed hospital discharges for patients needing rehabilitation in a postacute setting can exacerbate hospital-acquired mobility loss, prolong functional recovery, and increase costs. Systematic measurement of patient mobility by nurses early during hospitalization has the potential to help identify which patients are likely to be discharged to a postacute care facility versus home. To test the predictive ability of this approach, a machine learning classification tree method was applied retrospectively to a diverse sample of hospitalized patients (N = 761) using training and validation sets. Compared with patients discharged to home, patients discharged to a postacute facility were older (median, 64 vs 56 years old) and had lower mobility scores at hospital admission (median, 32 vs 41). The final decision tree accurately classified the discharge location for 73% (95%CI:67%-78%) of patients. This study emphasizes the value of systematically measuring mobility in the hospital and provides a simple decision tree to facilitate early discharge planning.
© 2019 Society of Hospital Medicine
Outcome and Predictors
Discharge location (postacute care facility vs home) was the primary outcome in this study, as recorded in a discrete field in the electronic medical record (EMR). To ensure the validity of this measure, we performed manual chart audits on a sample of patients (n = 300). It was confirmed that the measure entered in the discrete field in the EMR correctly identified the disposition (home vs postacute care facility) in all cases. The primary predictor was the lowest AM-PAC IMSF score obtained within 48 hours after hospital admission, reflecting the patient’s capability to mobilize after hospital admission. Raw scores were converted to scale scores (0-100) for analysis.9 Additional predictors considered included: age, sex, race, and primary diagnosis, all of which were readily available from the EMR at the time of hospital admission. We then grouped the primary diagnosis into the following categories using ICD-10 codes upon admission: Oncologic, Progressive Neurological, Sudden Onset Neurological, and Medical/Other.
Statistical Analysis
We constructed a classification tree, a machine learning approach,10 to predict discharge placement (postacute facility vs home) based on the patients’ hospital admission characteristics and AM-PAC IMSF score. The prediction model was developed using the classification tree approach, as opposed to a logistic regression model. This approach allows for the inclusion of higher-order interactions (ie, interactions of more than two predictors) which would need to be explicitly specified otherwise and a priori we did not have strong evidence from prior studies to guide the model construction. The classification tree was constructed and evaluated by dividing our sample into a 70% training set and a 30% validation set using random sampling within key strata defined by age (<65 vs ≥65 years), gender, and quartile of the AM-PAC IMSF score. The classification tree was developed using the training set. Next, measures of predictive accuracy (ie, the proportion of correctly classified patients with placement in a postacute facility [sensitivity]) and the proportion of correctly classified patients not discharged to postacute care (ie, to home, specificity), were estimated by applying the validation set to the classification tree. The R statistical package rpart11 with procedure rpart was used to construct the classification tree using standard criteria for growing (Gini index10) and pruning (misclassification error estimated by leave-1-out cross-validation12) the tree.
RESULTS