Hospital Medicine Update: High-Impact Literature from March 2018 to April 2019





To assist busy hospital medicine clinicians, we summarized 10 impactful articles from last year. The authors reviewed articles published between March 2018-April 2019 for the Hospital Medicine Updates at the Society of Hospital Medicine and the Society of General Internal Medicine Annual Meetings. The authors voted to select 10 of 30 presented articles based on quality and clinical impact for this summary. The key findings include: (1) Vancomycin or fidaxomicin are the first-line treatment for initial Clostridioides difficile infection; (2) Unnecessary supplemental oxygen is linked to increased mortality; aim for a target oxygen saturation of 90%-94% in most hospitalized patients; (3) Stigmatizing language in medical records impacts physician trainees’ attitudes and pain management practices; (4) Consider ablation for atrial fibrillation in patients with heart failure; (5) Patients with opioid use disorder should be offered buprenorphine or methadone therapy; (6) Apixaban is safe and may be preferable over warfarin in patients with atrial fibrillation and end-stage kidney disease; (7) It is probably safe to discontinue antimethicillin-resistant Staphylococcus aureus (MRSA) coverage in patients with hospital-acquired pneumonia who are improving and have negative cultures; (8) Selected patients with left-sided endocarditis (excluding MRSA) may switch from intravenous (IV) to oral antibiotics if they are clinically stable after 10 days; (9) Oral antibiotics may be equivalent to IV antibiotics in patients with joint and soft tissue infections; (10) A history–electrocardiogram–age–risk factors–troponin (HEART) score ≥4 is a reliable threshold for determining the patients who are at risk for short-term major adverse cardiac events and may warrant further evaluation.
© 2019 Society of Hospital Medicine
Given the breadth and depth of patients cared for by hospital medicine providers, it is challenging to remain current with the literature. The authors critically appraised the literature from March 2018 to April 2019 for high-quality studies relevant to hospital medicine. Articles were selected based on methodologic rigor and likelihood to impact clinical practice. Thirty articles were selected by the presenting authors for the Hospital Medicine Updates at the 2019 Society of Hospital Medicine (CH, CM) and Society of General Internal Medicine Annual Meetings (BS, AB). After two sequential rounds of voting and group discussion to adjudicate voting discrepancies, the authors selected the 10 most impactful articles for this review. Each article is described below with the key points summarized in the Table.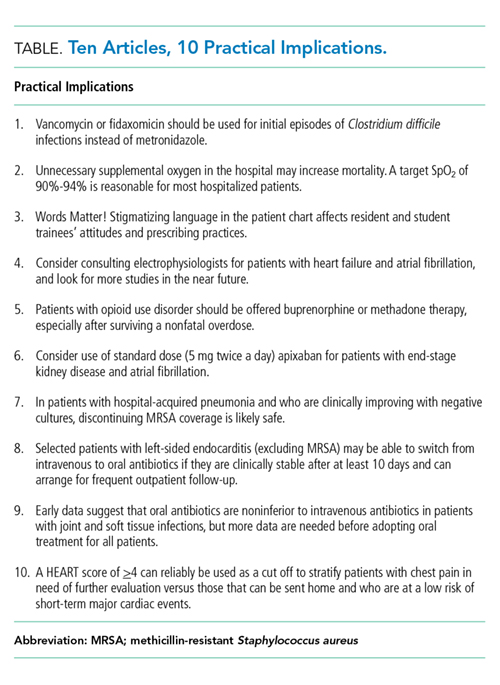
ESSENTIAL PUBLICATIONS
Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). McDonald LC, et al. Clin Infect Dis. 2018;66(7):e1–e48.1
Background. In the United States, approximately 500,000 Clostridioides difficile infections (CDI) occur annually with 15,000-30,000 deaths. CDI has become a marker of hospital quality and has been placed under numerous “pay for performance” metrics. The Infectious Diseases Society of America/Society of Healthcare Epidemiology of America updated their guidelines from 2010 regarding hospital surveillance, diagnostic testing, treatment, and infection precautions and control.
Findings. The panel included 14 multidisciplinary experts in epidemiology, diagnosis, infection control, and clinical management of adult and pediatric CDI. They used problem intervention comparison-outcome (PICO)-formatted, evidence-based questions. The selection of data and final recommendations were made in accordance with the GRADE criteria. A total of 35 recommendations were made.
Key clinical recommendations for hospitalists caring for adults: (1) Prescribe vancomycin or fidaxomicin over metronidazole for the initial treatment of CDI (strong recommendation, high quality of evidence); (2) Limit testing to the patients with unexplained new onset diarrhea, which is defined as greater than or equal to 3 unformed stools in 24 hours (weak recommendation, very low-quality evidence); (3) Avoid routine repeat testing within seven days, and only test asymptomatic patients for epidemiologic reasons (strong recommendation, moderate-quality evidence); (4) Minimize the frequency and duration of high-risk antibiotic therapy and the number of antibiotic agents prescribed (strong recommendation, moderate quality of evidence); (5) Discontinue therapy with the inciting antibiotic agent as soon as possible (strong recommendation, moderate quality of evidence).
Caveats. As with the clinical application of any guidelines, individual case adjustments may be required.