Perspectives of Clinicians, Staff, and Veterans in Transitioning Veterans from non-VA Hospitals to Primary Care in a Single VA Healthcare System





BACKGROUND: Veterans with healthcare needs utilize both Veterans Health Administration (VA) and non-VA hospitals. These dual-use veterans are at high risk of adverse outcomes due to the lack of coordination for safe transitions.
OBJECTIVES: The aim of this study was to understand the barriers and facilitators to providing high-quality continuum of care for veterans transitioning from non-VA hospitals to the VA primary care setting.
DESIGN: Guided by the practical robust implementation and sustainability model (PRISM) and the ideal transitions of care, we conducted a qualitative assessment using semi-structured interviews with clinicians, staff, and patients.
SETTING: This study was conducted at a single urban VA medical center and two non-VA hospitals.
PARTICIPANTS: A total of 70 participants, including 52 clinicians and staff (23 VA and 29 non-VA) involved in patient transition and 18 veterans recently discharged from non-VA hospitals, were included in this study.
APPROACH: Data were analyzed using a conventional content analysis and managed in Atlas.ti (Berlin, Germany).
RESULTS: Four major themes emerged where participants consistently discussed that transitions were delayed when they were not able to (1) identify patients as veterans and notify VA primary care of discharge, (2) transfer non-VA hospital medical records to VA primary care, (3) obtain follow-up care appointments with VA primary care, and (4) write VA formulary medications for veterans that they could fill at VA pharmacies. Participants also discussed factors involved in smooth transition and recommendations to improve care coordination.
CONCLUSIONS: All participants perceived the current transition-of-care process across healthcare systems to be inefficient. Efforts to improve quality and safety in transitional care should address the challenges clinicians and patients experience when transitioning from non-VA hospitals to VA primary care.
© 2020 Society of Hospital Medicine
METHODS
Study Design
We conducted a qualitative assessment within the VA Eastern Colorado Health Care System, an urban tertiary medical center, as well as urban and rural non-VA hospitals used by veterans. Semi-structured interview guides informed by the practical robust implementation and sustainability (PRISM) model, the Lean approach, and the Ideal Transitions of Care Bridge were used.25-27 We explored the PRISM domains such as recipient’s characteristics, the interaction with the external environment, and the implementation and sustainability infrastructure to inform the design and implementation of the intervention.25 The Lean approach included methods to optimize processes by maximizing efficiency and minimizing waste.26 The Ideal Transitions of Care Bridge was used to identify the domains in transitions of care such as discharge planning, communication of information, and care coordination.27
Setting and Participants
We identified the top 10 non-VA hospitals serving the most urban and rural veterans in 2015 using VA administrative data. Purposive sampling was used to ensure that urban and rural non-VA hospitals and different roles within these hospitals were represented. VA clinicians and staff were selected from the Denver VA Medical Center, a tertiary hospital within the Eastern Colorado Health Care System and one VA Community-Based Outpatient Clinic (CBOC) that primarily serves rural veterans. The Denver VA Medical Center has three clinics staffed by Patient Aligned Care Teams (PACTs), a model built on the concept of Patient-Centered Medical Home.28 Hospital leadership were initially approached for permission to recruit their staff and to be involved as key informants, and all agreed. To ensure representativeness, diversity of roles was recruited, including PACT primary care physicians, nurses, and other staff members such as medical assistants and administrators. Veterans were approached for sampling if they were discharged from a non-VA hospital during June–September 2015 and used the VA for primary care. This was to ensure that they remembered the process they went through postdischarge at the time of the interview.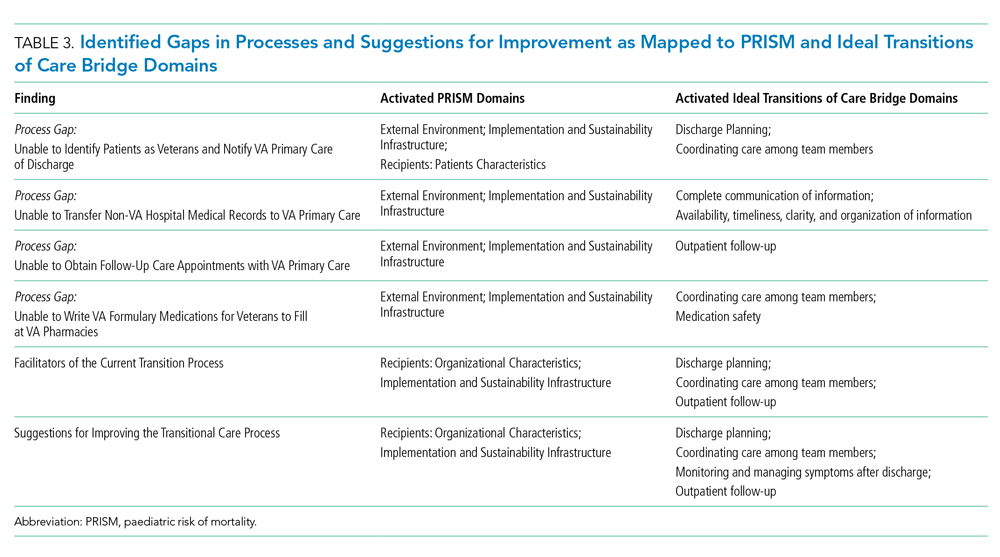
Data Collection and Analysis
The evaluation team members (RA, EL, and MM) conducted the interviews from November 2015 to July 2016. Clinicians, staff, and veterans were asked semi-structured questions about their experiences and their role in transitioning VA patients across systems (see Appendix for interview guides). Veterans were asked to describe their experience and satisfaction with the current postdischarge transition process. We stopped the interviews when we reached data saturation.29
Interviews were audio-recorded, transcribed verbatim, and validated (transcribed interviews were double-checked against recording) to ensure data quality and accuracy. Coding was guided by a conventional content analysis technique30, 31 using a deductive and inductive coding approach.31 The deductive coding approach was drawn from the Ideal Transitions of Care Bridge and PRISM domains. 32,33 Two evaluation team members (RA and EL) defined the initial code book by independently coding the first three interviews, worked to clarify the meanings of emergent codes, and came to a consensus when disagreements occurred. Next, a priori codes were added by team members to include the PRISM domains. These PRISM domains included the implementation and sustainability infrastructure, the external environment, the characteristics of intervention recipients, and the organizational and patient perspectives of an intervention.
Additional emergent codes were added to the code book and agreed upon by team members (RA, EL, and MM). Consistent with previously used methods, consensus building was achieved by identifying and resolving differences by discussing with team members (RA, EL, MM, CB, and RB).29 Codes were examined and organized into themes by team members.29,34-36 This process was continued until no new themes were identified. Results were reviewed by all evaluation team members to assess thoroughness and comprehensiveness.34,35 In addition, team members triangulated the findings with VA and non-VA participants to ensure validity and reduce researcher bias.29,37
