Impact of Preoperative Specialty Consults on Hospitalist Comanagement of Hip Fracture Patients





BACKGROUND: Hip fractures typically occur in frail elderly patients. Preoperative specialty consults, in addition to hospitalist comanagement, are often requested for preoperative risk assessment.
OBJECTIVE: Determine if preoperative specialty consults meaningfully influence management and outcomes in hip fracture patients, while being comanaged by hospitalists DESIGN: Retrospective cohort study
SETTING: Tertiary care hospital in Connecticut
PATIENTS: 491 patients aged 50 years and older who underwent surgery for an isolated fragility hip fracture, defined as one occurring from a fall of a height of standing or less.
INTERVENTION: Presence or absence of a preoperative specialty consult
MEASUREMENTS: Time to surgery (TTS), length of hospital stay (LOS), and postoperative complications
RESULTS: 177 patients had a preoperative specialty consult. Patients with consults were older and had more comorbidities. Most consult recommendations were minor (72.8%); there was a major recommendation only for eight patients (4.5%). Multivariate analysis demonstrates that consults are more likely to be associated with a TTS beyond 24 hours (Odds Ratio [OR] 4.28 [2.79-6.56]) and 48 hours (OR 2.59 [1.52-4.43]), an extended LOS (OR 2.67 [1.78-4.03]), and a higher 30-day readmission rate (OR 2.11 [1.09-4.08]). A similar 30-day mortality rate was noted in both consult and no-consult groups.
CONCLUSIONS: The majority of preoperative specialty consults did not meaningfully influence management and may have potentially increased morbidity by delaying surgery. Our data suggest that unless a hip fracture patient is unstable and likely to require active management by a consultant, such consults offer limited benefit when weighed against the negative impact of surgical delay.
© 2020 Society of Hospital Medicine
Our primary predictor was the presence or absence of a preoperative specialty consultation requested by the hospitalist. We also analyzed the following: covariates of demographics (age, sex, race), the ASA score, and severity of comorbidities using the Charlson comorbidity index (CCI) with a Quan modification;11 “R program package, International Classification of Disease (ICD)”12 was used to calculate the CCI using ICD-9 and ICD-10 diagnostic codes.
The primary outcome measures were TTS (measured in hours), LOS (measured in days), complications, and preoperative specialty consult resulting in a change in perioperative management. TTS was defined as the time elapsed from the presentation at the emergency department (ED) to surgery start. For transfer or direct admission patients, the time of admission was used in place of time of presentation. The measured complications included postoperative venous thromboembolic events, surgical site infection, myocardial infarction, stroke, and sepsis. Secondary outcome measures included 30-day mortality, readmission rate, and rate of return to OR. There were no elective or planned readmissions postoperatively on review of our institution’s orthopedic surgery registry.
Our team performed an extensive chart review including reviewing the admission note, consulting physician notes, and relevant test results. Our senior investigator (MK) then rated each preoperative specialty consult on appropriateness, the relative strength of the consultant’s recommendation, and resulting change in perioperative management. Cardiology consultations were deemed reasonable if a patient’s cardiac risk was considered elevated by the admitting physician or an active cardiac condition was present (suggestion of or clear evidence for acute coronary syndrome, acute congestive heart failure, uncontrolled arrhythmia, or symptomatic valvular disease). The determination of “elevated cardiac risk” was made, if admit note contained verbiage expressing concern for further evaluation for cardiac issues or words such as “high risk” or “elevated risk”. A specific guideline-based score such as the revised cardiac risk index was not consistently available in this retrospective chart review. A noncardiology consult was deemed reasonable only if it would have been warranted for the specific clinical situation—for example, a neurology consult for an acute stroke or a pulmonary consult for acute respiratory failure. Consult recommendations or outcomes were rated as minor, moderate, or major (see Table 1 for detailed criteria). Some consults may generate more than one recommendation, in these cases, we determined that a major recommendation supersedes a moderate or minor recommendation and only one was counted in the final analysis. Next we determined if a consult recommendation led to a change in perioperative or therapeutic management, defined as a medication or dosage change, need to delay surgery to stabilize an unstable medical condition, invasive procedures (such as thoracentesis or cardiac catheterization) or change in postoperative monitoring. As a way of clarification, a consult may have a minor recommendation such as an EKG but if no other recommendations were given and there was no change in therapeutic management such as a medication change, this would be considered as a “no change”.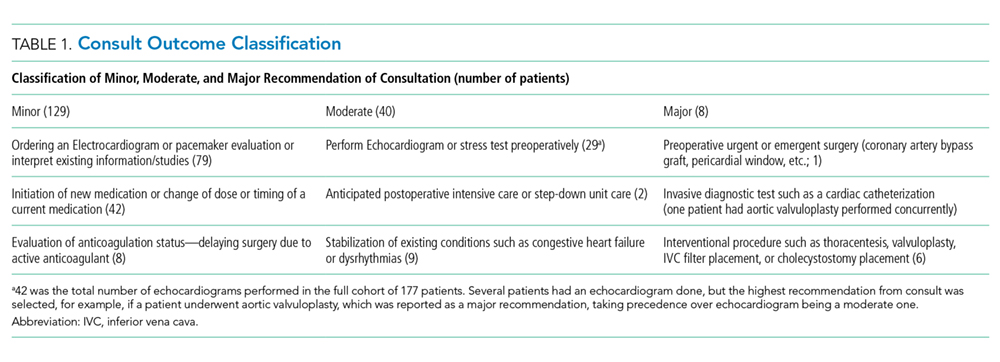
An independent rating of the entire dataset was subsequently performed by another hospitalist (KM) to establish interrater reliability. This reviewer was blinded to the initial rating and not involved in the initial design of the study or the data collection process. Because of the labor-intensive task of reviewing full charts, we followed a nonstandard process for interrater reliability. This rating was performed with the same dataset that was extracted by three members of our team (NB, SS, and MK); consequently, this does not account for variability in chart extraction as reiterated in the discussion.