Inpatient Communication Barriers and Drivers When Caring for Limited English Proficiency Children





BACKGROUND: Achieving effective communication between medical providers and families with limited English proficiency (LEP) in the hospital is difficult.
OBJECTIVE: Our objective was to identify barriers to and drivers of effective interpreter service use when caring for hospitalized LEP children from the perspectives of pediatric medical providers and interpreters.
DESIGN/ PARTICIPANTS/ SETTING: We used Group Level Assessment (GLA), a structured qualitative participatory method that allows participants to directly produce and analyze data in an interactive group session. Participants from a single academic children’s hospital generated individual responses to prompts and identified themes and relevant action items. Themes were further consolidated by our research team and verified by stakeholder groups.
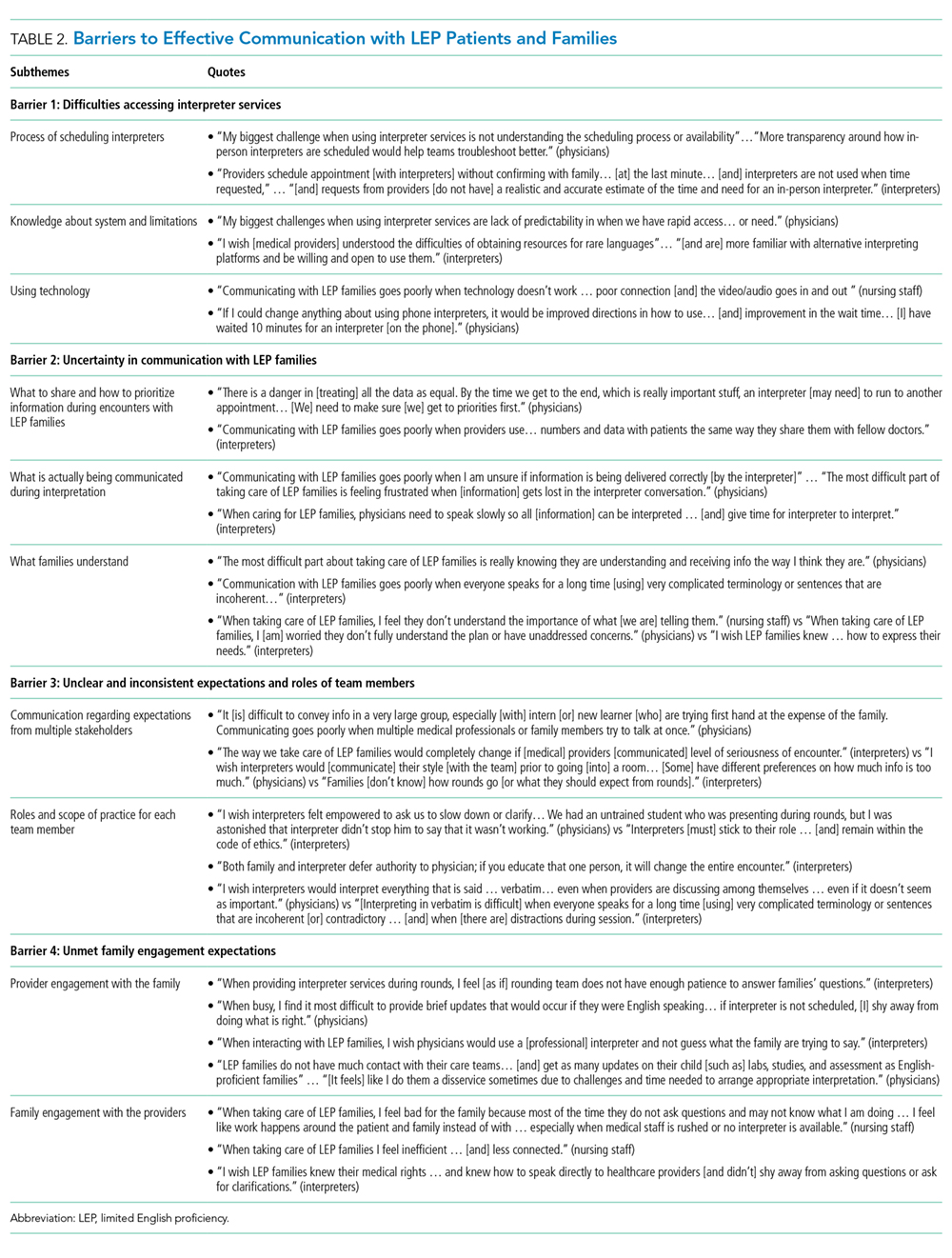
RESULTS: Four GLA sessions were conducted including 64 participants: hospital medicine physicians and pediatric residents (56%), inpatient nursing staff (16%), and interpreter services staff (28%). Barriers identified included: (1) difficulties accessing interpreter services; (2) uncertainty in communication with LEP families; (3) unclear and inconsistent expectations and roles of team members; and (4) unmet family engagement expectations. Drivers of effective communication were: (1) utilizing a team-based approach between medical providers and interpreters; (2) understanding the role of cultural context in providing culturally effective care; (3) practicing empathy for patients and families; and (4) using effective family-centered communication strategies.
CONCLUSIONS: Participants identified unique barriers and drivers that impact communication with LEP patients and their families during hospitalization. Future directions include exploring the perspective of LEP families and utilizing team-based and family-centered communication strategies to standardize and improve communication practices.
© 2019 Society of Hospital Medicine
Study Participants and Recruitment
Medical providers who care for hospitalized general pediatric patients were eligible to participate, including attending physicians, resident physicians, bedside nurses, and inpatient ancillary staff (eg, respiratory therapists, physical therapists). Interpreters employed by CCHMC with experience in the inpatient setting were also eligible. Individuals were recruited based on published recommendations to optimize discussion and group-thinking.15 Each participant was asked to take part in one GLA session. Participants were assigned to specific sessions based on roles (ie, physicians, nurses, and interpreters) to maximize engagement and minimize the impact of hierarchy.
Study Procedure
GLA involves a seven-step structured process (Appendix 1): climate setting, generating, appreciating, reflecting, understanding, selecting, and action.15,18 Qualitative data were generated individually and anonymously by participants on flip charts in response to prompts such as: “I worry that LEP families___,” “The biggest challenge when using interpreter services is___,” and “I find___ works well in providing care for LEP families.” Prompts were developed by study investigators, modified based on input from nursing and interpreter services leadership, and finalized by GLA facilitators. Fifty-one unique prompts were utilized (Appendix 2); the number of prompts used (ranging from 15 to 32 prompts) per session was based on published recommendations.15 During sessions, study investigators took detailed notes, including verbatim transcription of participant quotes. Upon conclusion of the session, each participant completed a demographic survey, including years of experience, languages spoken and perceived fluency,20 and ethnicity.
Data Analysis
Within each session, under the guidance of trained and experienced GLA facilitators (WB, HV), participants distilled and summarized qualitative data into themes, discussed and prioritized themes, and generated action items. Following completion of all sessions, analyzed data was compiled by the research team to determine similarities and differences across groups based on participant roles, consolidate themes into barriers and drivers of communication with LEP families, and determine any overlap of priorities for action. Findings were shared back with each group to ensure accuracy and relevance.
RESULTS
Participants
A total of 64 individuals participated (Table 1): hospital medicine physicians and residents (56%), inpatient nurses and ancillary staff (16%), and interpreters (28%). While 81% of physicians spoke multiple languages, only 25% reported speaking them well; two physicians were certified to communicate medical information without an interpreter present.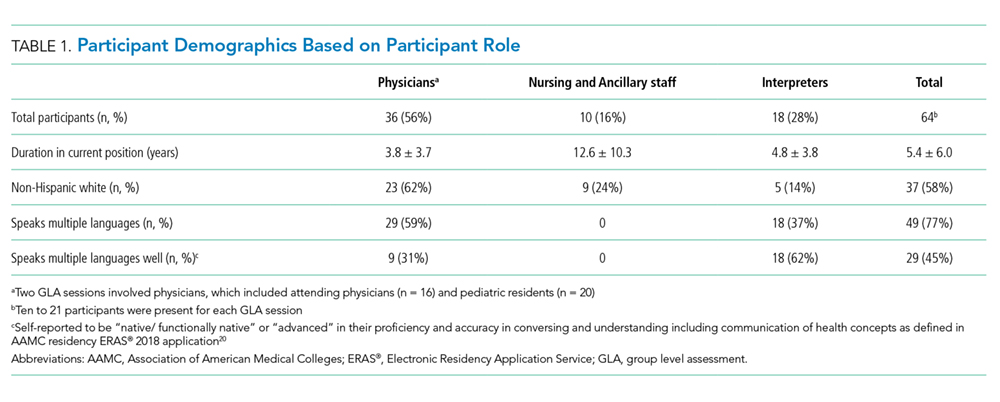
Themes Resulting from GLA Sessions
A total of four barriers (Table 2) and four drivers (Table 3) of effective communication with pediatric LEP patients and their families in the inpatient setting were identified by participants. Participants across all groups, despite enthusiasm around improving communication, were concerned about quality of care LEP families received, noting that the system is “designed to deliver less-good care” and that “we really haven’t figured out how to care for [LEP patients and families] in a [high-]quality and reliable way.” Variation in theme discussion was noted between groups based on participant role: physicians voiced concern about rapport with LEP families, nurses emphasized actionable tasks, and interpreters focused on heightened challenges in times of stress.