Reducing Unneeded Clinical Variation in Sepsis and Heart Failure Care to Improve Outcomes and Reduce Cost: A Collaborative Engagement with Hospitalists in a MultiState System





OBJECTIVE: To (1) measure hospitalist care for sepsis and heart failure patients using online simulated patients, (2) improve quality and reduce cost through customized feedback, and (3) compare patient-level outcomes between project participants and nonparticipants.
METHODS: We conducted a prospective, quasi-controlled cohort study of hospitalists in eight hospitals matched with comparator hospitalists in six nonparticipating hospitals across the AdventHealth system. We provided measurement and feedback to participants using Clinical Performance and Value (CPV) vignettes to measure and track quality improvement. We then compared length of stay (LOS) and cost results between the two groups.
RESULTS: 107 providers participated in the study. Over two years, participants improved CPV scores by nearly 8% (P < .001), with improvements in utilization of the three-hour sepsis bundle (46.0% vs 57.7%; P = .034) and ordering essential medical treatment elements for heart failure (58.2% vs 72.1%; P = .038). In study year one, average LOS observed/expected (O/E) rates dropped by 8% for participants, compared to 2.5% in the comparator group, equating to an additional 570 hospital days saved among project participants. In study year two, cost O/E rates improved from 1.16 to 0.98 for participants versus 1.14 to 1.01 in the comparator group. Based on these improvements, we calculated total cost savings of $6.2 million among study participants, with $3.8 million linked to system-wide improvements and an additional $2.4 million in savings attributable to this project.
CONCLUSIONS: CPV case simulation-based measurement and feedback helped drive improvements in evidence-based care that translated into lower costs and LOS, above-and-beyond other improvements at AdventHealth.
© 2019 Society of Hospital Medicine
Patient-Level Impact on LOS and Cost Per Case
We took advantage of the quasi-experimental design, in which only a portion of AdventHealth facilities participated in the project, to compare patient-level results from AQQP-participating physicians against the engagement-matched cohort of hospitalists at nonparticipating AdventHealth facilities. We adjusted for potential differences in patient-level case mix between the two groups by comparing the observed/expected (O/E) LOS and cost per case ratios for pneumonia/sepsis and heart failure patients.
At baseline, AQQP-hospitalists performed better on geometric LOS versus the comparator group (O/E of 1.13 vs 1.22; P = .006) but at about the same on cost per case (O/E of 1.16 vs 1.14; P = .390). Throughout the project, as patient volumes and expected per patient costs rose for both groups, O/E ratios improved among both AQQP and non-AQQP providers.
To set apart the contribution of system-wide improvements from the AQQP project-specific impacts, we applied the O/E improvement rates seen in the comparator group to the AQQP group baseline performance. We then compared that to the actual changes seen in the AQQP throughout the project to see if there was any additional benefit from the simulation measurement and feedback (Figure).
From baseline through year one of the project, the O/E LOS ratio decreased by 8.0% in the AQQP group (1.13 to 1.04; P = .004) and only 2.5% in the comparator group (1.22 to 1.19; P = .480), which is an absolute difference-in-difference of 0.06 LOS O/E. In year 1, these improvements represent a reduction in 892 patient days among patients cared for by AQQP-hospitalists of which 570 appear to be driven by the AQQP intervention and 322 attributable to secular system-wide improvements (Table 3). In year two, both groups continued to improve with the comparator group catching up to the AQQP group.
Geometric mean O/E cost per case also decreased for both AQQP (1.16 Baseline vs 0.98 Year 2; P < .001) and comparator physicians (1.14 Baseline vs 1.01 Year 2; P = .002), for an absolute difference-in-difference of 0.05 cost O/E. However, the AQQP-hospitalists showed greater improvement (15% vs 12%; P = .346; Table 3). As in the LOS analysis, the AQQP-specific impact on cost was markedly accelerated in year one, accounting for $1.6 million of the estimated $2.6 million total savings that year. Over the two-year project, these combined improvements drove an estimated $6.2 million in total savings among AQQP-hospitalists: $3.8 million of this appear to be driven by secular system effects and, based upon our quasi-experimental design, an additional $2.4 million of which are attributable to participation in AQQP.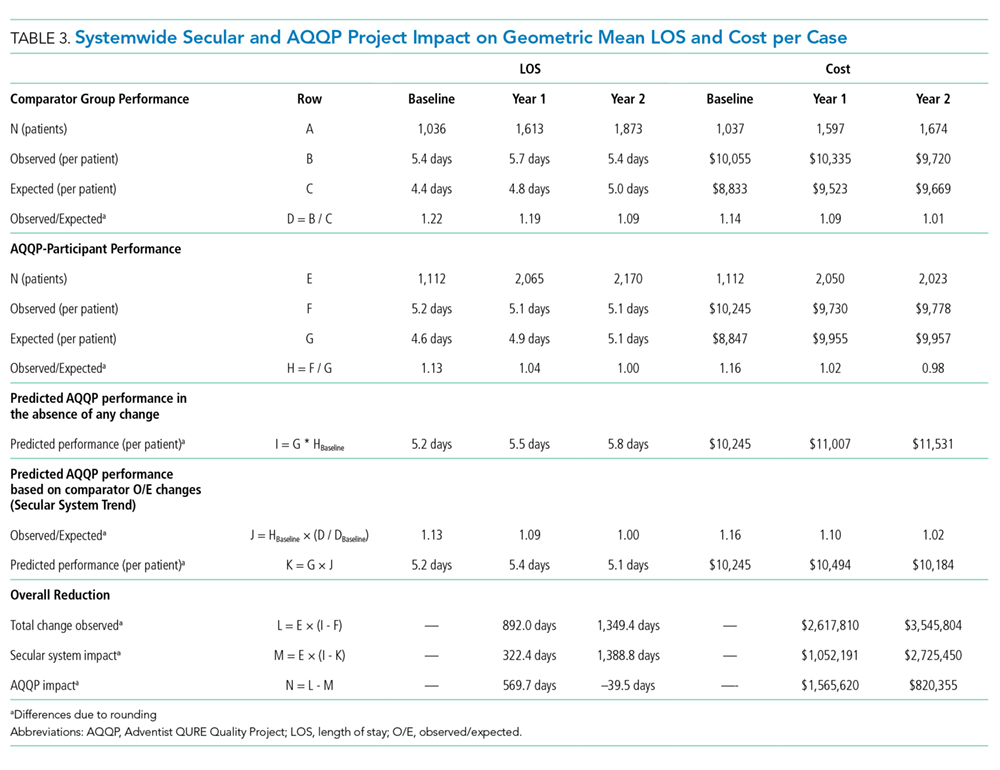
A Levene’s test for equality of variances on the log-transformed costs and LOS shows that the AQQP reductions in costs and LOS come from reduced variation among providers. Throughout the project, the standard deviation in LOS was reduced by 4.3%, from 3.8 days to 3.6 days (P = .046) and costs by 27.7%, from $9,391 to $6,793 (P < .001). The non-AQQP group saw a smaller, but still significant 14.6% reduction in cost variation (from $9,928 to $8,482), but saw a variation in LOS increase significantly by 20.6%, from 4.1 days to 5.0 days (P < .001).
