Documentation of Clinical Reasoning in Admission Notes of Hospitalists: Validation of the CRANAPL Assessment Rubric





OBJECTIVE: To establish a metric for evaluating hospitalists’ documentation of clinical reasoning in admission notes.
STUDY DESIGN: Retrospective study.
SETTING: Admissions from 2014 to 2017 at three hospitals in Maryland.
PARTICIPANTS: Hospitalist physicians.
MEASUREMENTS: A subset of patients admitted with fever, syncope/dizziness, or abdominal pain were randomly selected. The nine-item Clinical Reasoning in Admission Note Assessment & Plan (CRANAPL) tool was developed to assess the comprehensiveness of clinical reasoning documented in the assessment and plans (A&Ps) of admission notes. Two authors scored all A&Ps by using this tool. A&Ps with global clinical reasoning and global readability/clarity measures were also scored. All data were deidentified prior to scoring.
RESULTS: The 285 admission notes that were evaluated were authored by 120 hospitalists. The mean total CRANAPL score given by both raters was 6.4 (standard devision [SD] 2.2). The intraclass correlation measuring interrater reliability for the total CRANAPL score was 0.83 (95% CI, 0.76-0.87). Associations between the CRANAPL total score and global clinical reasoning score and global readability/clarity measures were statistically significant (P < .001). Notes from academic hospitals had higher CRANAPL scores (7.4 [SD 2.0] and 6.6 [SD 2.1]) than those from the community hospital (5.2 [SD 1.9]), P < .001.
CONCLUSIONS: This study represents the first step to characterizing clinical reasoning documentation in hospital medicine. With some validity evidence established for the CRANAPL tool, it may be possible to assess the documentation of clinical reasoning by hospitalists.
© 2019 Society of Hospital Medicine
RESULTS
The admission notes of 120 hospitalists were evaluated (Table 1). A total of 39 (33%) physicians were moonlighters with primary appointments outside of the hospitalist division, and 81 (68%) were full-time hospitalists. Among the 120 hospitalists, 48 (40%) were female, 60 (50%) were international medical graduates, and 90 (75%) were of nonwhite race. Most hospitalist physicians (n = 47, 58%) had worked in our health system for less than five years, and 64 hospitalists (53%) devoted greater than 50% of their time to patient care.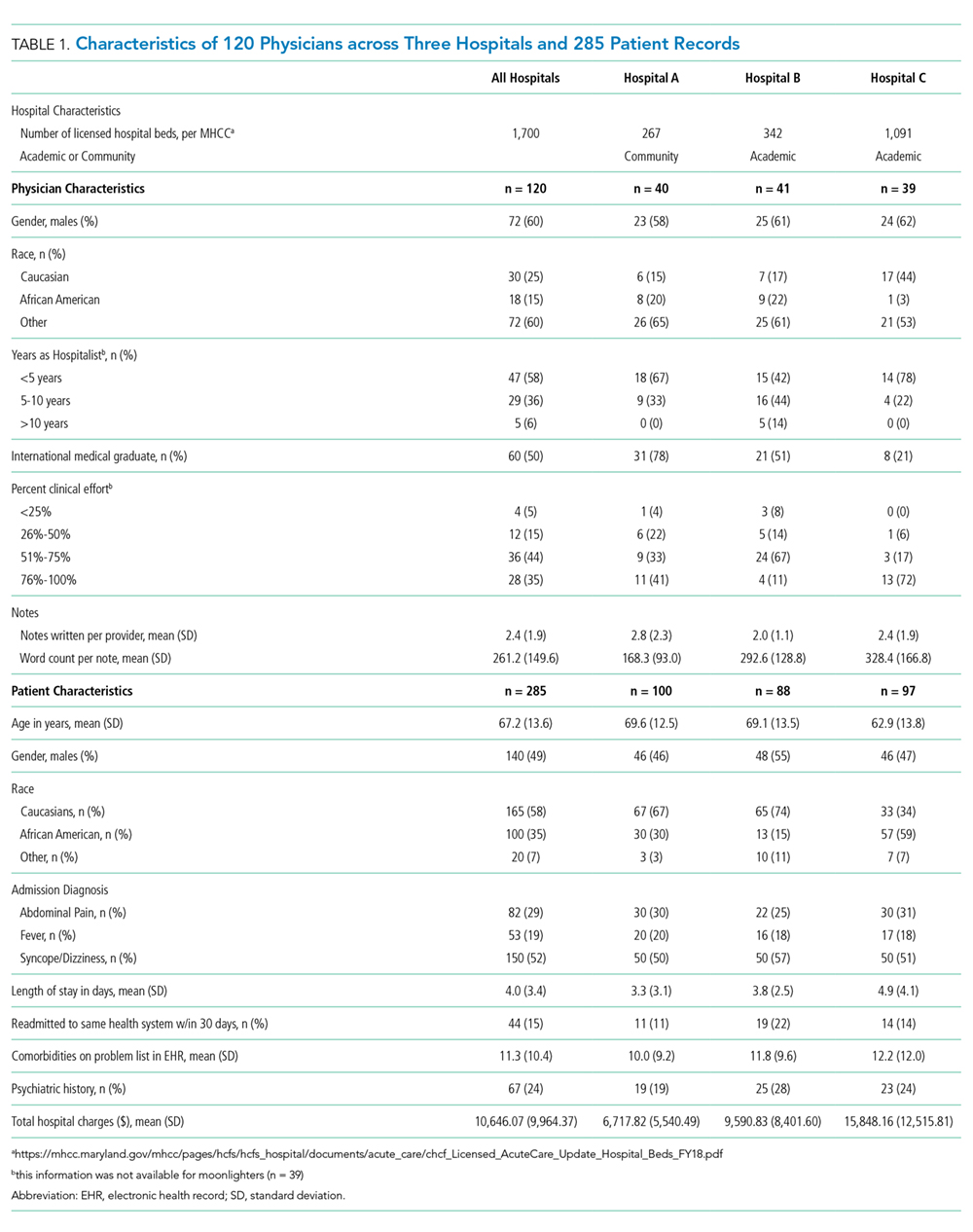
Approximately equal numbers of patient admission notes were pulled from each of the three hospitals. The average age of patients was 67.2 (SD 13.6) years, 145 (51%) were female, and 120 (42%) were of nonwhite race. The mean LOS for all patients was 4.0 (SD 3.4) days. A total of 44 (15%) patients were readmitted to the same health system within 30 days of discharge. None of the patients died during the incident hospitalization. The average charge for each of the hospitalizations was $10,646 (SD $9,964).
CRANAPL Data
Figure 1 shows the distribution of the scores given by each rater for each of the nine items. The mean of the total CRANAPL score given by both raters was 6.4 (SD 2.2). Scoring for some items were high (eg, summary statement: 1.5/2), whereas performance on others were low (eg, estimating LOS: 0.1/1 and describing the potential need for upgrade in care: 0.0/1).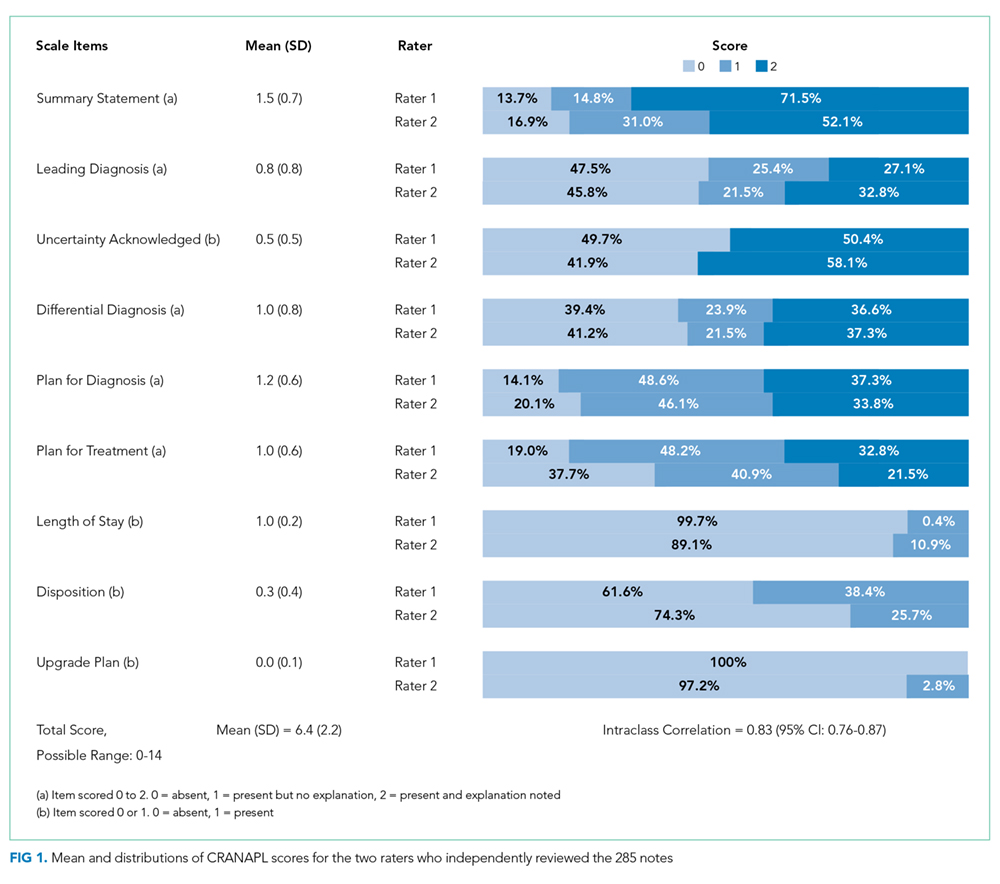
Validity of the CRANAPL Tool’s Internal Structure
Cronbach’s alpha, which was used to measure internal consistency within the CRANAPL tool, was 0.43. The ICC, which was applied to measure the interrater reliability for both raters for the total CRANAPL score, was 0.83 (95% CI: 0.76-0.87). The ICC values for intrarater reliability for raters 1 and 2 were 0.73 (95% CI: 0.60-0.83) and 0.73 (95% CI: 0.45-0.86), respectively.
Relations to Other Variables Validity
Associations between CRANAPL total scores, global clinical reasoning, and global scores for note readability/clarity were statistically significant (P < .001), Figure 2.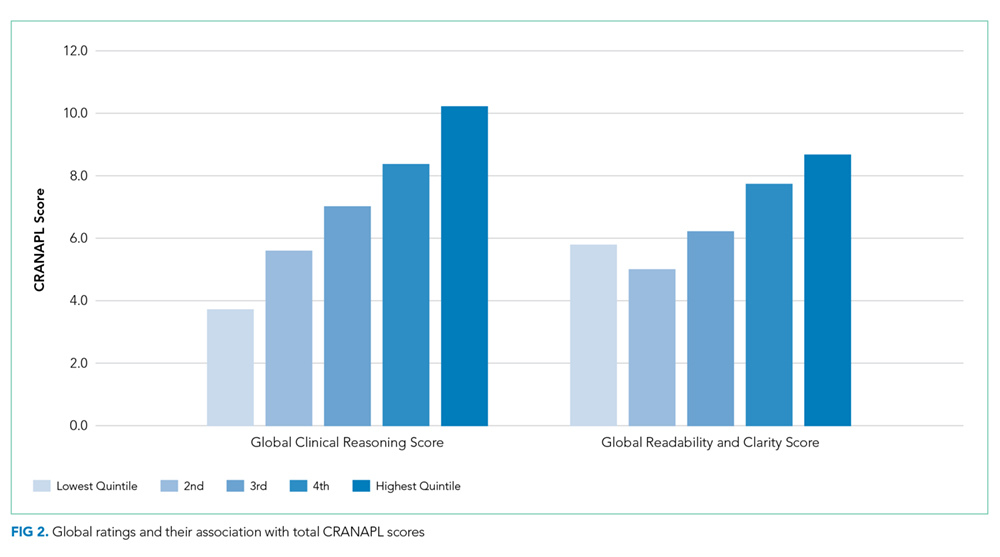
Eight out of nine CRANAPL variables were statistically significantly different across the three hospitals (P <. 01) when data were analyzed by hospital site. Hospital C had the highest mean score of 7.4 (SD 2.0), followed by Hospital B with a score of 6.6 (SD 2.1), and Hospital A had the lowest total CRANAPL score of 5.2 (SD 1.9). This difference was statistically significant (P < .001). Five variables with respect to admission diagnoses (uncertainty acknowledged, differential diagnosis, plan for diagnosis, plan for treatment, and upgrade plan) were statistically significantly different across notes. Notes for syncope/dizziness generally yielded higher scores than those for abdominal pain and fever.
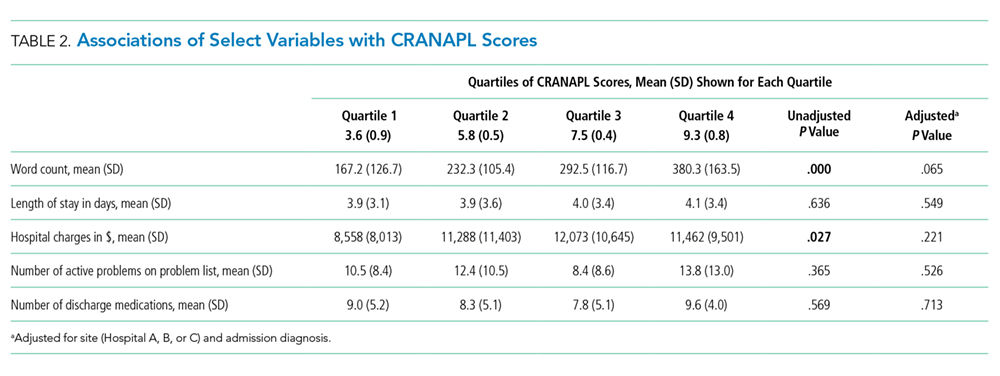
Factors Associated with High CRANAPL Scores
Table 2 shows the associations between CRANAPL scores and several covariates. Before adjustment, high CRANAPL scores were associated with high word counts of A&Ps (P < .001) and high hospital charges (P < .05). These associations were no longer significant after adjusting for hospital site and admitting diagnoses.