Preventing Delirium Takes a Village: Systematic Review and Meta-Analysis of Delirium Preventive Models of Care





BACKGROUND: Each hospital day of delirium incurs greater healthcare costs, higher levels of care, greater staff burden, and higher complication rates. Accordingly, administrators are incentivized to identify models of care that reduce delirium rates and associated costs.
PURPOSE: We present a systematic review and meta-analysis of delirium prevention models of care.
DATA SOURCES: Ovid MEDLINE, CINAHL, Cochrane Database of Systematic Reviews, EMBASE, and PsycINFO.
STUDY SELECTION: Eligible models of care were defined as provider-oriented interventions involving revision of professional roles, multidisciplinary teams, and service integration. Included studies implemented multidomain, multicomponent interventions, used a validated delirium instrument, and enrolled a control group to evaluate efficacy or effectiveness.
DATA EXTRACTION: We extracted data on study design, population, model of care, outcomes, and results.
DATA SYNTHESIS: A total of 15 studies were included. All but two studies reported reduction in delirium or its duration, and 11 studies reported statistically significant improvements. Using random effects models, the pooled odds ratios of delirium incidence were 0.56 (95% CI: 0.37-0.85) from three randomized controlled trials, 0.63 (95% CI 0.37-1.07) from four pre–post intervention studies, and 0.79 (95% CI: 0.46-1.37) from three additional nonrandomized studies.
CONCLUSIONS: Several models of care can prevent delirium. In general, higher quality studies were more likely to demonstrate statistical significance of an effect. The diverse models of care included here explored interventions adapted to specific care settings, especially by addressing setting-specific delirium risk factors. These care models illustrate a range of promising strategies that deserve growing recognition, refinement, and implementation.
© 2019 Society of Hospital Medicine
Study Characteristics
The 15 studies that met the inclusion criteria are summarized in the Table.18-32 Delirium prevention was among the primary outcomes of 13 studies; delirium outcomes were reported in the other two studies as well, which were primarily designed to assess feasibility.26,27 Six studies were conducted in the United States, three in Sweden, two in Spain, two in the United Kingdom, and one each conducted in Korea and Canada. Healthcare settings among the included studies involved the intensive care unit (six studies), medical floors (four studies), surgical floors (three studies), a long-term care unit (one study), and
Outcomes Reported
All but one of the studies reported delirium incidence. The most commonly used delirium screening instrument was the Confusion Assessment Method (CAM) or its modified version, the CAM-ICU (11 studies).33,34 Other methods used to assess mentation included the Richmond Agitation Sedation Scale,35 the Organic Brain Syndrome scale,36 the revised Delirium Rating Scale,37 the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition,38 and the Confusion Rating Scale.39 (Details regarding delirium screening tools can be found in the systematic review by De and Wand.40) Researchers performed delirium assessment in nine studies, whereas assessments were performed by clinical staff in the remaining studies. Other outcomes reported included length of stay (LOS), mortality, number of days ventilated, and functional decline. None of the included studies reported cost effectiveness.
Risk of Bias Assessment
Risk of bias assessment identified only two studies—both randomized controlled trials—as low risk (Table). The remaining studies had moderate (four studies) or high risk (nine studies).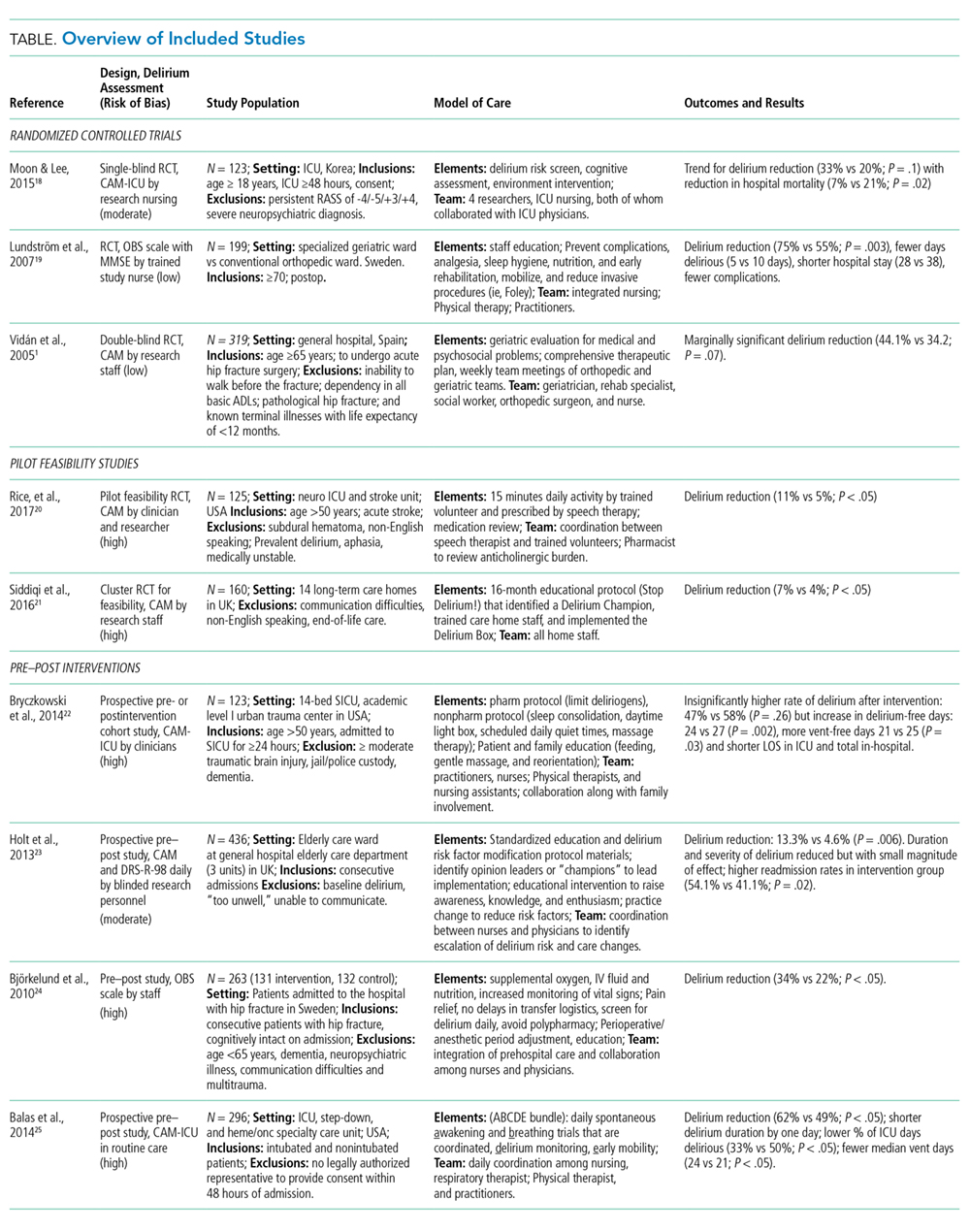
Results from Individual Studies
Of the 15 studies, nine reported a statistically significant reduction in delirium incidence, and another two reported a statistically insignificant reduction. In addition, seven of the eight studies that assessed delirium duration found reduced duration in the intervention cohort, and two of the three studies that reported delirium severity found a reduction in the intervention group.
Results of Meta-Analysis
Random effects models were created to meta-analyze groups of studies based on design as follows: randomized controlled trials (three studies18,19,25), pre–post intervention studies (four of six studies included28-31), and other nonrandomized studies (three of four studies included21-23). Meta-analysis was not completed for the two feasibility studies26,27 because delirium outcome data were limited due to the feasibility study design. The study of Dale et al.32 was excluded from the meta-analysis because the rates of CAM-ICU completion differed substantially between control and intervention groups (0.35 vs 1.49 per 24 hours, respectively), leading to imbalanced between-group sensitivity in delirium detection and Needham et al.20 was also excluded because it reported only days of delirium, not delirium incidence. The study by Lundström et al.24 was also excluded from the meta-analysis because delirium incidence was measured on days 1, 3, and 5, whereas the other studies reported delirium daily.
