How Much Time are Physicians and Nurses Spending Together at the Patient Bedside?





BACKGROUND: Bedside rounding involving both nurses and physicians has numerous benefits for patients and staff. However, precise quantitative data on the current extent of physician–nurse (MD–RN) overlap at the patient bedside are lacking.
OBJECTIVE: This study aimed to examine the frequency of nurse and physician overlap at the patient beside and what factors affect this frequency.
DESIGN: This is a prospective, observational study of time-motion data generated from wearable radio frequency identification (RFID)-based locator technology.
SETTING: Single-institution academic hospital.
MEASUREMENTS: The length of physician rounds, frequency of rounds that include nurses simultaneously at the bedside, and length of MD–RN overlap were measured and analyzed by ward, day of week, and distance between patient room and nursing station.
RESULTS: A total of 739 MD rounding events were captured over 90 consecutive days. Of these events, 267 took place in single-bed patient rooms. The frequency of MD–RN overlap was 30.0%, and there was no statistical difference between the three wards studied. Overall, the average length of all MD rounds was 7.31 ± 0.58 minutes, but rounding involving a bedside nurse lasted longer than rounds with MDs alone (9.56 vs 5.68 minutes, P < .05). There was no difference in either the length of rounds or the frequency of MD–RN overlap between weekdays and weekends. Finally, patient rooms located farther away from the nursing station had a lower likelihood of MD–RN overlap (Pearson’s r = –0.67, P < .05).
CONCLUSION: RFID-based technology provides precise, automated, and high-throughput time-motion data to capture nurse and physician activity. At our institution, 30.0% of rounds involve a bedside nurse, highlighting a potential barrier to bedside interdisciplinary rounding.
© 2019 Society of Hospital Medicine
Rounding Characteristics over the Course of the Week
To assess how rounding characteristics differed over the work week, we partitioned our data into the individual days of the week. The length of each MD rounding event (time spent in each patient room) did not vary significantly over the course of the week (Figure 2a). When the data for the individual days were aggregated into “weekdays” (Monday through Friday) and “weekends” (Saturday and Sunday), the mean lengths of MD rounds were 7.26 ± 0.32 minutes on weekdays and 7.47 ± 0.52 minutes on weekends (P > .05).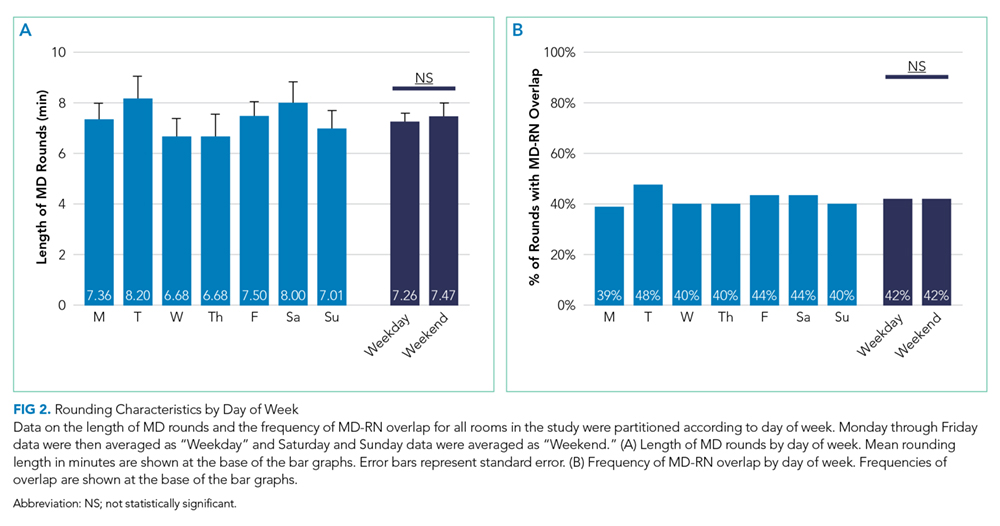
In addition, there was no difference in how frequently physicians and nurses overlapped at the patient bedside between weekdays and weekends. Of the 565 weekday MD rounding events, 238 had a nurse at bedside (42.1%), and of the 173 weekend MD rounding events, 73 had a nurse at bedside (42.2%; Figure 2b).
Effect of a Bedside Nurse on the Length of Rounds
Next, the data on the length of MD rounds were partitioned based on whether there was a bedside nurse present during rounds. The mean length of rounds with only MDs (without a bedside nurse) was 5.68 ± 0.24 minutes. By comparison, the mean length of rounds with both a nurse and a physician at the patient bedside was 9.56 ± 0.53 minutes (Figure 3). This difference was statistically significant (P < .001).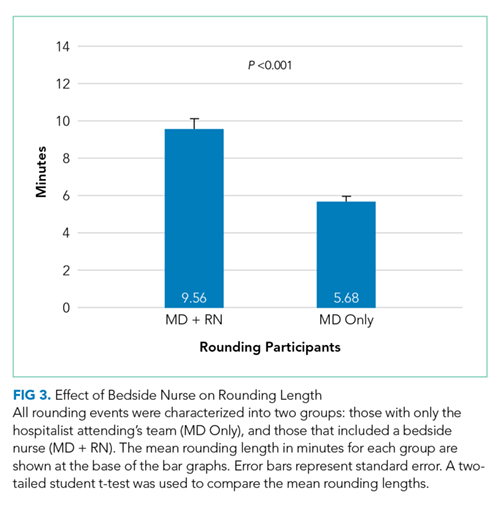
Association between Patient Room Location and the Likelihood of MD–RN Overlap
All three wards in this study have a linear layout, consisting of 19 patient rooms in a row (Figure 4a). The nursing station is located in a central position within each ward, across from the 10th patient room. The frequency of MD–RN overlap was calculated for each room, and each room was ranked according to its relative distance from the nursing station. For each individual ward, there was no statistically significant trend in MD–RN overlap frequency as a function of the distance to the nursing station (data not shown). However, when the data from all three wards were aggregated, there was a statistically significant trend (P < .05) with a negative Pearson correlation (r = –0.670; Figure 4b). The slope of the best fit line was 1.94, suggesting that for each additional room farther away from the nursing station, the likelihood of interdisciplinary rounds (with both physicians and nurses together at the bedside) decreases by almost 2%.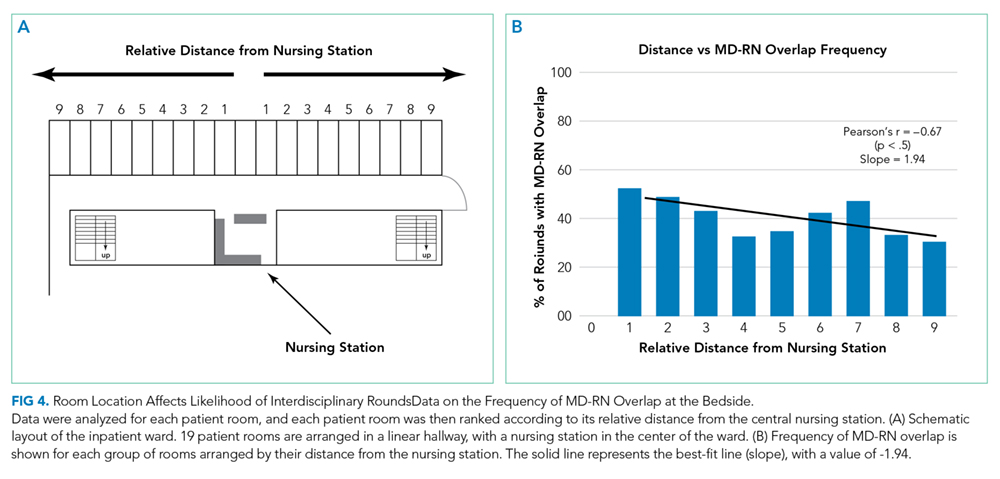
DISCUSSION
To the best of our knowledge, this is the first time-motion study of MD–RN overlap using real-time, RFID-based location technology to capture the rounding activity of both nurses and physicians. Our primary interest was to examine the extent of MD–RN overlap at the patient bedside. This is an important metric that can pave the way for bedside interdisciplinary rounds. Although the exact nature of nurse-physician communication was not measured using the methodology in this study, understanding the length of time physicians spend in patient rooms, across different wards and throughout the work week, provides insights on the current workflow and potential areas of improvement. For example, we found that 30.0% of MD rounds overlapped with a nurse at the bedside. This baseline data highlight one potential barrier to institution-wide bedside interdisciplinary rounds. Workflow changes, such as better co-localization of patients by service lines or utilization of technologies to augment the visibility of rounding physicians, may improve this overlap frequency.